

Abstract
Context.
Breast cancer survivors (BCS) face adverse physical and psychological symptoms, often co-occurring. Biologic and psychological factors may link symptoms within clusters, distinguishable by prevalence and/or severity. Few studies have examined the effects of behavioral interventions or treatment of symptom clusters.
Objectives.
The aim of this study was to identify symptom clusters among post-treatment BCS and determine symptom cluster improvement following the Mindfulness-Based Stress Reduction for Breast Cancer (MBSR(BC)) program.
Methods.
Three hundred twenty-two Stage 0–III post-treatment BCS were randomly assigned to either a six-week MBSR(BC) program or usual care. Psychological (depression, anxiety, stress, and fear of recurrence), physical (fatigue, pain, sleep, and drowsiness), and cognitive symptoms and quality of life were assessed at baseline, six, and 12 weeks, along with demographic and clinical history data at baseline. A three-step analytic process included the error-accounting models offactor analysis and structural equation modeling.
Results.
Four symptom clusters emerged at baseline: pain, psychological, fatigue, and cognitive. From baseline to six weeks, the model demonstrated evidence of MBSR(BC) effectiveness in both the psychological (anxiety, depression, perceived stress and QOL, emotional well-being) (P = 0.007) and fatigue (fatigue, sleep, and drowsiness) (P < 0.001) clusters. Results between six and 12 weeks showed sustained effects, but further improvement was not observed.
Conclusion.
Our results provide clinical effectiveness evidence that MBSR(BC) works to improve symptom clusters, particularly for psychological and fatigue symptom clusters, with the greatest improvement occurring during the six-week program with sustained effects for several weeks after MBSR(BC) training.
Trial Registration.
Name and URL of Registry: ClinicalTrials.gov. Registration number: NCT01177124.
Keywords: Breast cancer, Mindfulness-Based Stress Reduction (MBSR), symptom cluster, physical symptoms, psychological symptoms, post-treatment
Introduction
Breast cancer is expected to affect one-in-eight women during her lifetime.1 Even with advances in cancer treatments and decreased mortality rates,2 breast cancer remains a major public health concern3 in part because of the multiple debilitating symptoms as a result of surgery, chemotherapy, radiation therapy, and/or biologic therapy.4 Often, breast cancer survivors (BCS) are plagued by adverse physical (fatigue, pain, and sleep disturbances) and psychological symptoms (stress, anxiety, alteration in cognitive functioning, depression, and fear of recurrence [FOR]) that may remain and/or occur years after treatment completion,5 reducing both quality of life and functionality.6–8
Although BCS suffer from multiple adverse symptoms, fatigue is reported to be the most debilitating,9,10 often lasting up to 10 years after diagnosis.11 Pain is reported by up to 33% of BCS after curative therapy.9 The prevalence of sleep disturbances are reported to be twice as high among BCS in comparison with the general population.12,13
It is estimated that up to 70% of cancer survivors experience six or more co-occurring symptoms.14 With this prevalence, there is increasing evidence to support examining symptom clusters among BCS to improve effective therapies.15,16 The term “symptom cluster” was defined over a decade ago as multiple concurrent and related symptoms that are not required to have shared etiology.17 Evidence of specific symptom clusters among BCS were reported in the following: psychological/mood symptoms in seven studies,5,16,18–22 fatigue emerged as a cluster in six studies,5,18–22 somatic or physical symptoms (e.g., pain) emerged in four studies,18–20,23 gastrointestinal symptoms emerged in three studies,5,16,24 sleep disturbance emerged in two studies,18,22 and cognitive impairment emerged in two studies.21,24 A hormonal cluster observed by Roiland and Heidrich18 is the only cluster without a match in other symptom cluster studies. Although the mechanism for symptom clusters is not completely understood, it has been suggested that biologic mechanisms18 and psychological factors, such as stress,19,25 may link symptoms together within clusters, distinguishable by prevalence and/or severity.
Although pharmacologic and psychological treatments are used to treat symptoms, few have examined the treatment of symptom clusters.20 Nonpharmacologic complementary and alternative medicine therapies, such as Mindfulness-Based Stress Reduction (MBSR),23 hold promise as a clinical treatment for the reduction of multiple co-occurring symptoms among BCS. Evidence supports MBSR as an effective clinical treatment for reducing individual symptoms of fatigue and mood disturbance,21 depression and anxiety,22,24,26 and FOR.22
Although this is the first large trial assessing the effects of MBSR(BC) across multiple symptom clusters in BCS, in our previous trial among 84 BCS, within-group symptom cluster improvement occurred after the MBSR(BC) program5 using the M.D. Anderson Symptom Inventory.27 Three clusters emerged: gastrointestinal, cognitive/psychological, and fatigue.5 A limitation of this past study was the small sample size, resulting in insufficient power to detect between-group effects and preventing implementation of a more robust statistical method, such as structural equation modeling. Therefore, this current trial corrects for this limitation by implementing error-accounting models of factor analysis and structural equation modeling to allow for tests of symptom cooccurrence and tests of treatment effects within the same model. The aim of this study was to identify symptom clusters among post-treatment BCS and test whether these symptom clusters improved following the MBSR(BC) program at the six- and 12-week follow-up compared with usual care (UC). This purpose fits well with the central aim of this clinical trial: to determine the efficacy of MBSR(BC) in improving outcomes.
Methods
Sample and Setting
Three hundred twenty-two (n = 322) BCS aged ≥ 21 years, with a diagnosis of Stage 0–III BC and within two weeks to two years off treatment were recruited from the Moffitt Cancer Center, Carol and Frank Morsani Center for Advanced Healthcare, and the Life Hope Medical Group, located in Tampa, FL. Exclusion criteria included a diagnosis of Stage IV BC, severe mental disorder, and/or BC recurrence.
Procedures
Study Design and Randomization.
A two-armed randomized controlled design was used to randomize 322 BCS to the MBSR(BC) program or UC. Randomization was stratified by type of surgery (lumpectomy vs. mastectomy), adjuvant BC treatment (chemotherapy with or without radiation vs. radiation alone), and stage of BC (Stage 0/I vs. II/III).
Recruitment and Data Collection Procedures.
The study protocol was approved by the Institutional Review Board at the University of South Florida and scientific review committee at the Moffitt Cancer Center. BCS meeting inclusion criteria and if interested in the study were invited to an orientation session during which informed consent was obtained along with baseline assessments followed by randomization. At baseline and at six and 12 weeks, demographic data, clinical history, measures of psychological and physical symptoms, and QOL were collected.
MBSR(BC) Intervention.
The MBSR(BC) program, modeled after the MBSR program developed by Jon Kabat-Zinn et al.,28,29 was adapted to assist breast cancer patients in taking an active role in stress reduction and symptom management through the self-regulatory process of meditation.22 The MBSR(BC) intervention consists of three components: 1) educational material related to relaxation, meditation, the mind-body connection, and a healthy lifestyle for survivors, 2) practice of meditation in group meetings and homework assignments, and 3) group processes related to barriers to the practice of meditation and supportive group interaction.30
A psychologist trained in MBSR taught the six-week, two-hour per week sessions that included training in formal meditation techniques (sitting meditation, body scan, gentle Hatha yoga, and walking meditation), along with informal techniques of integrating mindfulness into daily life activities. BCS were requested to formally and informally practice the meditative techniques for 15–45 minutes per day and to record their practice times in a daily diary. A manual and compact discs were provided to guide home practice.
Fidelity.
Intervention sessions conducted by a single instructor were monitored weekly by a research assistant, who recorded time and delivery of the components of the two-hour class sessions on a fidelity checklist.
Usual Care.
UC participants continued standard post-treatment clinic visits and were asked to refrain from practicing meditation, yoga techniques, and MBSR(BC) during study enrollment. They were offered the MBSR(BC) intervention within six months after completion of the study.
Measures
Demographic Data and Clinical History.
Demographic data on age, ethnicity, educational achievement, marital status, income, and employment status and clinical history data on cancer type, date of diagnosis, and treatments were collected at baseline and updated at six and 12 weeks.
Symptoms
Worry and Fear of Cancer Recurrence.
The Concerns About Recurrence Scale31 consists of two subscales: overall FOR and nature of FOR. Higher scores demonstrate greater overall fear and worry.31 Concerns About Recurrence Scale has shown good reliability (0.87) and validity for breast cancer subjects.31
Depression.
The Center for Epidemiological Studies Depression Scale measured depressive symptomatology during the past week32 and measures frequency of depressive feelings and behaviors. A reliability coefficient of 0.92 has been reported for breast cancer subjects32 and satisfactory validity has been demonstrated in many studies across different populations.33,34
Anxiety.
State-Trait Anxiety Inventory35 was used to measure “state” or situational anxiety. The state anxiety subscale includes 20 items that measure present anxiety. It has reported high internal consistency (0.95) and convergent validity with other measures of anxiety.35
Perceived Stress.
The Perceived Stress Scale36 was used to assess how often in the past month the subject appraised life situations as “stressful.” The scale has demonstrated both good reliability (0.84–0.86) and good validity.36
Mindfulness.
Cognitive and Affective Mindfulness Scale-Revised measured mindfulness37 and measures four domains: attention, present-focus, awareness, and acceptance/nonjudgment. It has demonstrated an acceptable level of internal consistency (alpha 0.74–0.77) and evidence of convergent and discriminant validity with other measures of mindfulness.37
Symptom Severity.
Symptom severity was measured using the M.D. Anderson Symptom Inventory, which measures the severity of symptoms and the degree that they may interfere with daily functioning. It has demonstrated satisfactory consistency (≥0.85) and test-retest reliability (≥0.76).38
Sleep Quality.
Sleep quality was measured by the Pittsburgh Sleep Quality Index,39 which measures seven domains of sleep: quality, latency, duration, efficiency, disturbances, use of sleep medications, and daytime sleep function. It has demonstrated adequate reliability ranging from 0.70 to 0.78 for sleep disturbance.39
Fatigue.
Fatigue was measured using the Fatigue Symptom Inventory,40 which evaluates the perceived level of fatigue by assessing the perceived severity, frequency, and interference with daily functioning. It was found to have good internal consistency, with alpha coefficients greater than 0.90.40
Pain.
Pain was measured by the Brief Pain Inventory,41 which examines pain intensity and interference. Higher scores are associated with greater pain severity and interference. It has demonstrated reliability coefficients from 0.82 to 0.95.41
Cognitive Functioning.
The Everyday Cognition (ECog) scale is a multidimensional instrument measuring impairment and change of everyday functioning relevant to several neuropsychological domains.42 The scale provides a global score and six subscales including everyday memory, language, visuo-spatial abilities, planning, organization, and divided attention. It has reported adequate reliability (0.82) and convergent validity and external validity.42
Health-Related Quality of Life.
Health-related QOL was measured by the Medical Outcomes Studies Short-Form General Health Survey (SF-36),43 which has eight subscales that assess physical functioning, physical role functioning, bodily pain, general health, vitality, social functioning, emotional role functioning, and mental health. Estimates of reliability range from 0.62 to 0.94 in different study populations, and most scores have exceeded 0.80. Test-retest reliability estimates range from 0.43 to 0.90.43
Statistical Analyses
A three-step analytic process was used to assess the central aim of this study. Each step adopted a latent variable approach. The first step was to identify the clustering of symptoms using baseline data (before randomization to the MBSR(BC) program). Exploratory factor analysis was used to identify which measures or items within measures “clustered” together. Multiple combinations of measures and items were tested. The model with the lowest Bayesian Information Criterion was selected. This model was tested at each additional time point using root mean square error of approximation (RMSEA), comparative fit index (CFI), and the standardized root mean square residual (SRMR). When the CFI coefficient was greater than 0.95, the RMSEA less than 0.07, and the SRMR less than 0.08, the model fit was considered acceptable.44,45
The second step of the analysis used a conditional structural equation model to test the beneficial effects of MBSR(BC) at six weeks (immediately post-MBSR(BC) training). Using intent-to-treat principles in this model, MBSR(BC) was tested as a moderator of symptom cluster improvement (using the latent variables established in the factor analysis of Step 1). RMSEA, CFI, and the SRMR were used to evaluate model fit.
The third analytic step was to test for the follow-up effects of MBSR(BC). For this step, the same structural equation modeling (SEM) strategy was used as identified in Step 2 with symptom cluster improvement measured from six weeks to 12 weeks. Although this approach (splitting the baseline to six weeks and six weeks to 12 weeks) was not ideal, we did not have sufficient power to run a growth curve model with multiple latent variables and a treatment moderator.
Model estimation was conducted in Mplus, v. 7.146 using full information maximum likelihood estimation to benefit from all available information in the data. That is, participants with missing information were included in the analyses under the assumption of missing at random (i.e., missingness conditional on observed variables).
Results
Participant Characteristics
Three hundred twenty-two BCS were enrolled in the study, with 299 completing. There were no statistically significant differences between groups at baseline. The mean age was 56.6yearsand the majority were white non-Hispanic (69.4%), married (64.4%), diagnosed with Stage II BC (35.7%), and received a mastectomy (53.4%) and radiation and chemotherapy (35.7%). For additional demographics, clinical history characteristics, and CONSORT data, refer to Lengacher et al.47
Step 1 Results
This trial included several measurements of each symptom, and different combined measures were tested to establish the best symptom cluster arrangement or grouping in the factor analysis. The model with the best fit (lowest Bayesian Information Criterion) resulted in four clusters at baseline that included: 1) a pain cluster with the SF-36 pain scale and the Brief Pain Inventory Severity Scale, 2) a psychological cluster with state anxiety (State-Trait Anxiety Inventory), depression (Center for Epidemiological Studies Depression), emotional well-being (SF-36), and stress (Perceived Stress Scale), 3) a fatigue cluster with fatigue (Fatigue Symptom Inventory), sleep (Pittsburgh Sleep Quality Index), and drowsiness (M.D. Anderson Symptom Inventory), and 4) a cognitive cluster with memory (ECog) and mindfulness (Cognitive and Affective Mindfulness Scale-Revised). This model was considered acceptable using CFI = 0.97, RMSEA = 0.069, and SRMR = 0.05. Figure 1 depicts a diagram of this model. Tables 1–4 display the mean scores of each measure composing the clusters by random assignment. The arrows in Figure 1 point toward the indicators that assessed each symptom cluster. The coefficients attached to each arrow represent standardized beta weights, which indicate the strength of the relationship between the measure and the cluster. Because the acceptability of this model was supported, the identical structure was used to test the MBSR(BC) effects at all three time points (baseline, six weeks, and 12 weeks). Although pain is often viewed as a single symptom and not a traditional symptom cluster, in this trial it was evaluated as a latent variable in the factor analysis because multiple dimensions of pain were measured.
Fig. 1.
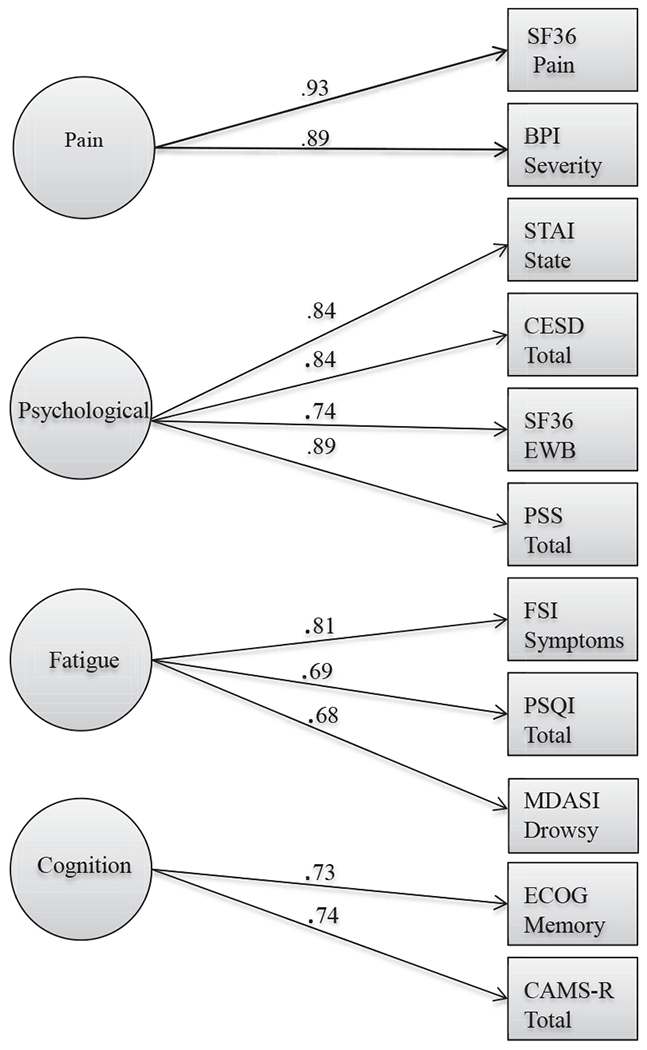
Baseline confirmatory factor analysis. Latent variables (clusters) are presented within circles. The measures that compose the clusters are presented in squares. Arrows and standardized beta weights indicate the linkages. All beta weights between measures and symptom clusters were statistically significant (P < 0.001).
Table 1.
Mean Symptom Scores by Random Assignment and Time Point for Each Measure Comprising the Psychological Cluster
| MBSR(BC) |
UC |
|||||
|---|---|---|---|---|---|---|
| Cluster Psychological | Mean | SD | n | Mean | SD | n |
| Depression (CESD) | ||||||
| Baseline | 10.87 | 6.89 | 167 | 10.04 | 6.46 | 155 |
| Week 6 | 8.12 | 5.45 | 154 | 8.82 | 6.05 | 146 |
| Week 12 | 8.66 | 6.26 | 155 | 8.95 | 6.80 | 148 |
| Anxiety (STAI) | ||||||
| Baseline | 38.62 | 12.30 | 167 | 35.86 | 11.29 | 155 |
| Week 6 | 30.62 | 12.80 | 159 | 31.76 | 13.20 | 152 |
| Week 12 | 31.82 | 12.10 | 155 | 32.99 | 13.40 | 148 |
| Stress (PSS) | ||||||
| Baseline | 17.57 | 7.71 | 167 | 15.39 | 7.62 | 155 |
| Week 6 | 20.19 | 5.06 | 156 | 20.21 | 5.33 | 151 |
| Week 12 | 12.90 | 7.75 | 158 | 12.89 | 8.20 | 154 |
| Emotional well-being (SF-36) | ||||||
| Baseline | 63.83 | 17.42 | 167 | 68.57 | 18.32 | 155 |
| Week 6 | 70.87 | 18.02 | 152 | 69.36 | 18.78 | 145 |
| Week 12 | 71.33 | 19.41 | 153 | 72.71 | 19.13 | 146 |
MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; UC = usual care; CESD = Center for Epidemiological Studies Depression Scale; PSS = Perceived Stress Scale; STAI = State-Trait Anxiety Inventory; SF-36 = Short-Form General Health Survey.
Table 4.
Mean Symptom Reports by Random Assignment and Time Point for Each Measure Comprising the Cognition Cluster
| MBSR(BC) |
UC |
|||||
|---|---|---|---|---|---|---|
| Cluster Cognition | Mean | SD | n | Mean | SD | n |
| Memory (ECog) | ||||||
| Baseline | 1.75 | .88 | 37 | 1.65 | .74 | 35 |
| Week 6 | 1.47 | .71 | 34 | 1.51 | .74 | 34 |
| Week 12 | 1.41 | .68 | 32 | 1.50 | .72 | 34 |
| Mindfulness (CAMS-R) | ||||||
| Baseline | 34.02 | 6.61 | 167 | 35.37 | 7.17 | 155 |
| Week 6 | 35.20 | 7.55 | 154 | 36.71 | 7.52 | 146 |
| Week 12 | 35.63 | 10.53 | 161 | 35.30 | 11.40 | 155 |
MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; UC = usual care; ECog = Everyday Cognition; CAMS-R = Cognitive and Affective Mindfulness Scale-Revised.
Step 2 Results
To test whether the UC or MBSR(BC) group differed before the intervention, the experimental condition was tested as a covariate for the best-fitting cluster model at baseline. Even with the covariate added, model fit remained adequate (CFI = 0.97, RMSEA = 0.066, and SRMR = 0.05). Evidence emerged of a potential baseline group difference on the psychological cluster (anxiety, depression, perceived stress, and emotional well-being) (P < 0.05). The remaining clusters did not differ statistically (all P’s > 0.05). As a result of the difference in the psychological cluster, the decision was made to account for baseline values using difference scores for all outcomes at the six-week and 12-week time points. To determine if the symptom cluster model established at baseline remained an acceptably fitting model using difference scores, the baseline to six-week difference scores were tested using confirmatory factor analysis. The model fit remained acceptable. In fact, fit indices improved somewhat (CFI = 0.99, RMSEA = 0.03, and SRMR = 0.05). When the model was tested conditionally with experimental assignment used as a covariate, MBSR(BC) demonstrated evidence of effectiveness. Improvement in both the psychological (anxiety, depression, perceived stress and QOL, emotional well-being) (P = 0.007) and fatigue (fatigue, sleep, and drowsiness) (P < 0.001) clusters were related to assignment. Specifically, participants who received the MBSR(BC) training improved more than those who did not at the six-week time point. The standardized regression coefficients (β) for psychological symptoms (.17) and fatigue (.24) correspond with Cohen’s d effect sizes of 0.35 and 0.50, respectively. These are considered medium-sized effects. Pain (P = 0.97) and cognition (memory and mindfulness) (P = 0.78) cluster improvement was not related to assignment. Figure 2 diagrams the six-week model conditional on experimental assignment. Tables 1–4 display the mean scores of each measure composing the clusters by random assignment.
Fig. 2.
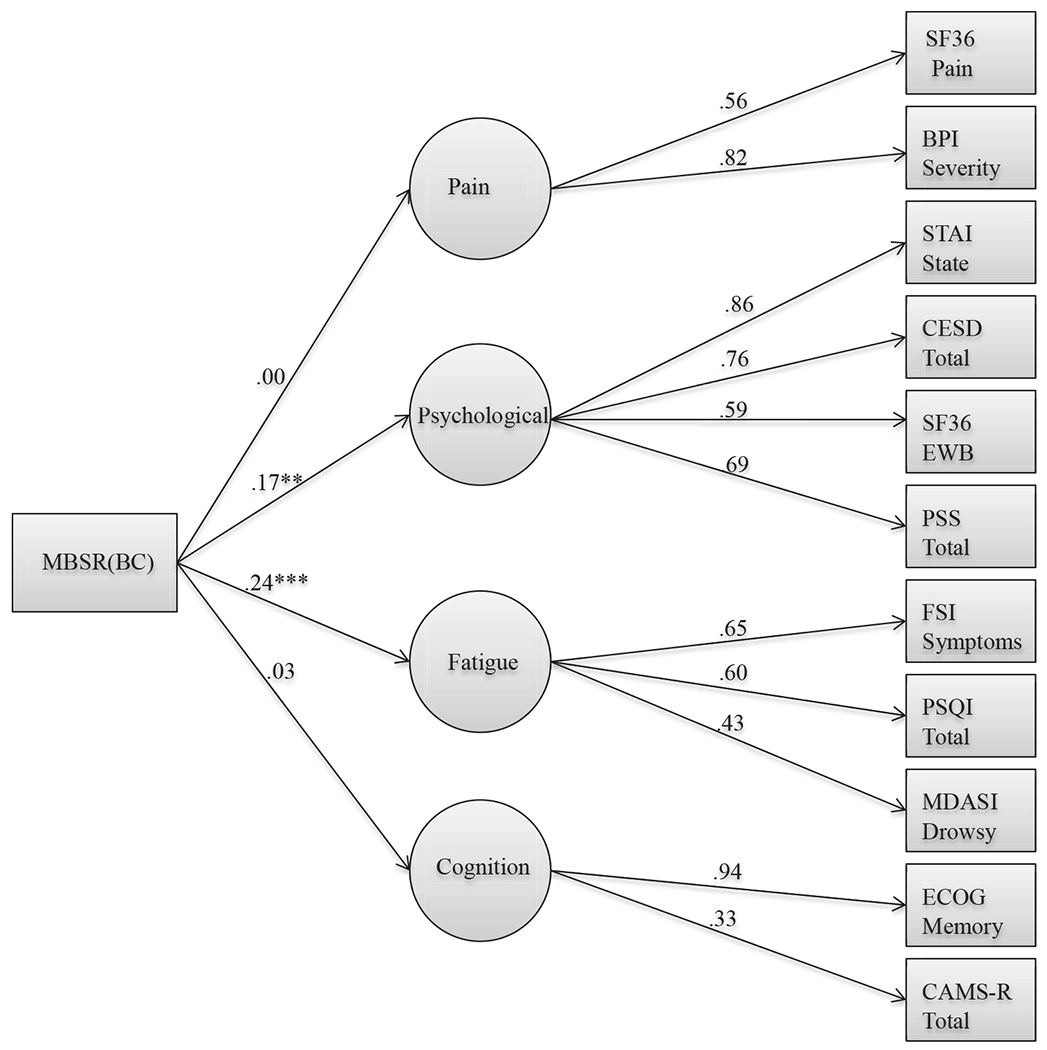
Six-week structural equation model. Confirmatory factor analysis model is the same as baseline. The measured variables were quantified using difference squares between baseline and six weeks to control for initial levels. Experimental assignment is represented in the MBSR(BC) box. Arrows and standardized beta weights from this box represent MBSR(BC)’s relationship to symptom improvement: **P < 0.01; ***P = 0.001. All beta weights between measures and symptom clusters were statistically significant (P < 0.001). BPI = Brief Pain Inventory; CAMS-R = Cognitive and Affective Mindfulness Scale-Revised; CESD = Center for Epidemiological Studies Depression; ECog = Everyday Cognition; FSI = Fatigue Symptom Inventory; MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; MDASI = M.D. Anderson Symptom Inventory; PSS = Perceived Stress Scale; PSQI = Pittsburgh Sleep Quality Index; SF-36 = Short-Form General Health Survey; STAI = State-Trait Anxiety Inventory.
Step 3 Results
To determine whether improvement continued between the end of MBSR(BC) training (six weeks) and the 12-week follow-up point, the same initial factor analytic model was tested using difference scores between six and 12 weeks (Fig. 3). Although the fit indices for this model were not as good as the six-week model, they remained acceptable (CFI = 0.96, RMSEA = 0.04, and SRMR = 0.05). When tested conditionally on experimental condition, general symptom cluster improvement did not vary (psychological, P = 0.84; fatigue, P = 0.80; cognition, P = 0.26; and pain, P = 0.09). It is important to note that a lack of MBSR(BC)-related improvement on the 12-week difference scores does not mean that the observed six-week improvement disappeared. Rather, it means that the degree of improvement between those time points was not contingent on MBSR(BC). Tables 1–4 display the mean scores of each measure composing the clusters by random assignment.
Fig. 3.
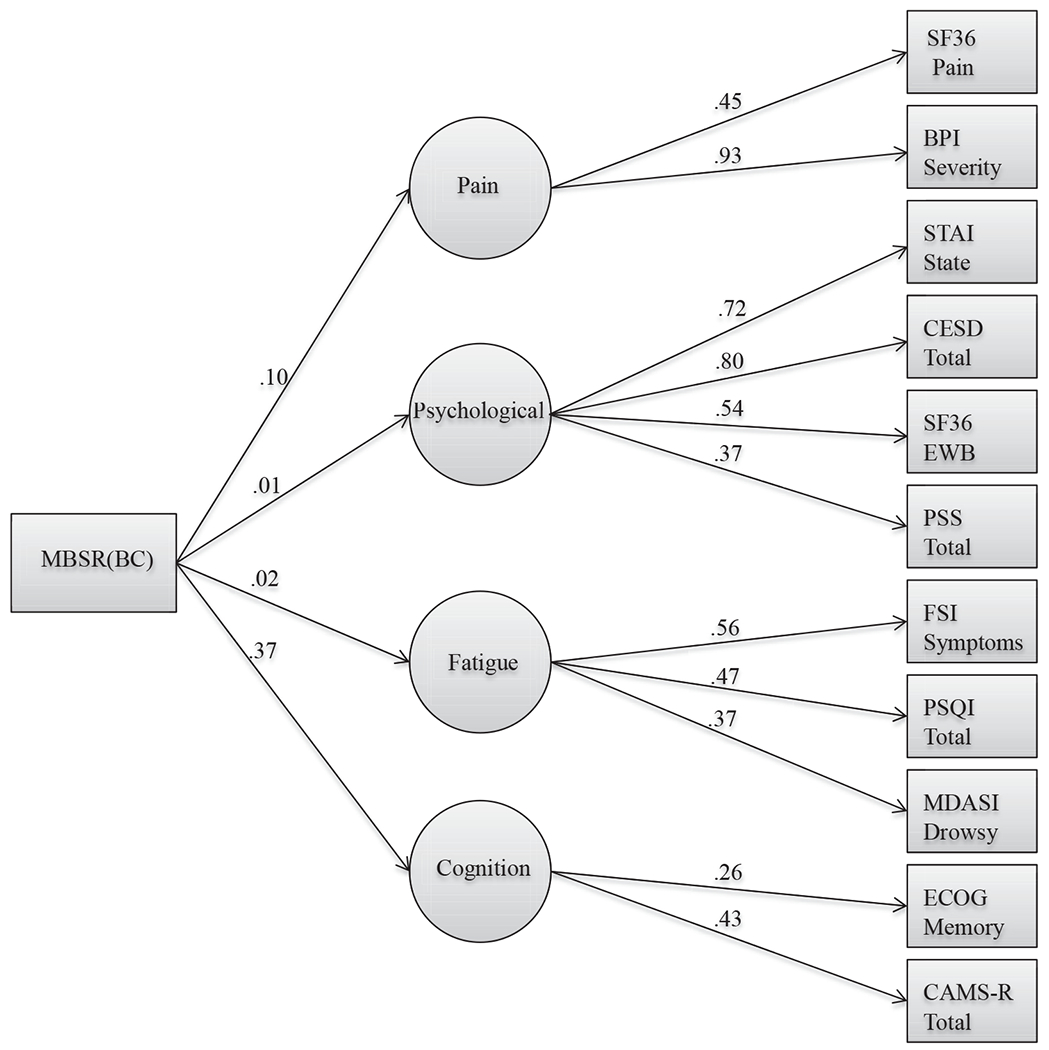
Six- to 12-week structural equation model. Confirmatory factor analysis model is the same as baseline. The measured variables were quantified using difference scores from six weeks to 12 weeks to control for initial levels. Experimental assignment is represented in the MBSR(BC) box. Arrows and standardized beta weights from this box represent MBSR(BC)’s relationship to symptom improvement. All beta weights between measures and symptom clusters were statistically significant (P < 0.001). BPI = Brief Pain Inventory; CAMS-R = Cognitive and Affective Mindfulness Scale-Revised; CESD = Center for Epidemiological Studies Depression; ECog = Everyday Cognition; FSI = Fatigue Symptom Inventory; MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; MDASI = M.D. Anderson Symptom Inventory; PSS = Perceived Stress Scale; PSQI = Pittsburgh Sleep Quality Index; SF-36 = Short-Form General Health Survey; STAI = State-Trait Anxiety Inventory.
Discussion
This study is the first identified clinical trial that tested the effects of MBSR(BC) across multiple symptom clusters in post-treatment BCS. Building on our previous symptom cluster research, this current trial used multiple specific symptom measures to define the clusters. It also tested whether reduction in the symptom cluster experience were the result of the MBSR(BC) program and assessed whether the symptom cluster reductions continued at 12 weeks.
This study also aimed to advance symptom cluster research and research on effective clinical treatment of symptom clusters among BCS by use of an effective nonpharmacologic intervention. Our results identified that immediate symptom cluster improvement occurred during the six-week MBSR(BC) training period, and although it generally did not increase after the six-week time point, improvements were generally sustained to 12 weeks.
The results of this trial first support the existence of multiple symptom clusters among post-treatment BCS. The symptom clusters that emerged replicated the two most commonly occurring symptom clusters in the literature: psychological symptoms and fatigue symptoms5,18–20,22,24 and two other clusters also were observed in multiple studies: pain symptoms18–21 and cognitive symptoms.22,26 The existence of these co-existing symptoms suggests, for example, a patient experiencing fatigue may also experience drowsiness, resulting from sleep disruption. In addition, BCS who experience depression may also experience stress and anxiety, affecting emotional well-being. Although previous research has explored clustering of symptoms, few have focused solely on BCS.
A second significant outcome of this trial was evidence that the MBSR(BC) intervention had a positive effect on the improvement of BCS-specific symptom clusters, the psychological and fatigue clusters, with medium-sized effects (Cohen’s d = 0.34 and 0.50, respectively). Clinically, this is an important finding that MBSR(BC) not only improves individual symptoms but concurrently is improving “clusters” of symptoms. There are no identified studies testing MBSR across multiple symptom clusters in post-treatment BCS, for comparison. This current trial supports the effectiveness of MBSR(BC) in reducing fatigue in BCS, as reported in our preliminary study.5 One surprising outcome was that differences between groups were not observed in the “cognitive” cluster, which included a measure of mindfulness. However, this was not a “mindfulness” cluster, as a mindfulness measure shared sufficient variance with a “memory” measure to create the latent variable labeled the “cognitive” cluster. Other studies should directly measure whether mindfulness improved in our participants using the multiple measures of mindfulness used in this study.
Although a component of all models tested, statistically significant differences between MBSR(BC) and UC were not observed with the pain cluster. In previous studies, the effect of MBSR on pain symptoms has not been absolute but has been shown to vary based on pain condition.48 In the case of our sample of early-stage cancer survivors, pain reports were relatively low compared with other cancer samples with more advanced stage patients49 introducing the possibility that our study was not sensitive enough to detect pain symptom reductions.
A third major outcome of this trial was that symptom cluster improvement occurred predominately during the period of time of the six-week MBSR(BC) training. Although improvements did not diminish from six to 12 weeks, they did not differ between six-week and 12-week follow-up assessment, possibly because of floor effects. By the end of the six weeks, participants did not report high levels of symptoms, restricting the range of potential improvement that could possibly be observed at the 12-week time point. Again, there are no other comparison research studies examining the effects of MBSR(BC) on symptom clusters.
Potential Clinical Implications and Directions for Future Research
This large randomized trial provides evidence that physical, psychological, and cognitive symptom clusters exist among post-treatment BCS. Our results indicate that the symptom clusters identified at baseline were sustained for 12 weeks, with an immediate benefit within the training period. Clinically, this study provides evidence for clinicians to assess and screen for individual and clinically aligned related symptoms and determine if interventions like MBSR(BC) can be offered to improve multiple individual symptoms and clusters of symptoms. Future research should continue to evaluate MBSR(BC)’s effectiveness among more diverse populations, and other cancer populations, along with examining related biologic mechanisms of action of MBSR(BC).
Limitations
Although the three-step approach used in this study allowed for the observation of different effects at six and 12 weeks, a full growth curve model could have tested for curvilinear effects across all three time points. Unfortunately, using the latent variable approach of SEM, there was insufficient power to implement such a longitudinal model. Additionally, the cognitive cluster supported by the factor analyses should be interpreted cautiously. The ECog measure, which was a key component of the cognitive symptom cluster, was only administered to a subsample of our trial. The relationships observed for the cognitive cluster can be considered preliminary data for future work.
Conclusions
In conclusion, the findings from this trial are an encouraging step toward expanding survivorship care to meet the needs of the growing BCS population. Understanding symptom clusters in cancer survivors may result in greater therapeutic benefits by integrating treatments for concurrent symptoms, thus improving QOL.50 In addition to QOL, multiple symptoms also affect prognosis and functional status of those with cancer.51 The practice of complementary and alternative medicine therapies, such as MBSR(BC), show promise on a potentially large scale, for self-management of the multiple co-occurring adverse symptoms often experienced by BCS.
Previous research reports symptom clusters to vary according to cancer type,52 disease stage,52 and treatment type.53 This trial adds to this existing evidence specific to BCS. It provides evidence that clusters of symptoms exist among BCS and identifies MBSR(BC) as an effective nonpharmacologic intervention, having the most improvement in the psychological and fatigue clusters, with the greatest benefit occurring during the six-week MBSR(BC) training. This study also demonstrated that although there were no additional improvements at 12 weeks, the improvements were sustained to 12 weeks.
Table 2.
Mean Symptom Reports by Random Assignment and Time Point for Each Measure Comprising the Fatigue Cluster
| MBSR(BC) |
UC |
|||||
|---|---|---|---|---|---|---|
| Cluster Fatigue | Mean | SD | n | Mean | SD | n |
| Fatigue (FSI) | ||||||
| Baseline | 16.39 | 8.75 | 167 | 14.48 | 8.36 | 155 |
| Week 6 | 12.33 | 7.59 | 152 | 13.38 | 8.45 | 145 |
| Week 12 | 12.20 | 8.56 | 152 | 13.27 | 8.71 | 147 |
| Sleep (PSQI) | ||||||
| Baseline | 9.12 | 5.04 | 165 | 8.25 | 4.23 | 155 |
| Week 6 | 7.26 | 4.47 | 148 | 7.52 | 4.11 | 145 |
| Week 12 | 7.08 | 4.42 | 150 | 7.02 | 4.12 | 145 |
| Drowsiness (MDASI) | ||||||
| Baseline | 3.14 | 3.10 | 167 | 2.92 | 3.14 | 155 |
| Week 6 | 2.32 | 2.46 | 152 | 2.61 | 2.97 | 145 |
| Week 12 | 2.16 | 2.85 | 152 | 2.33 | 2.78 | 147 |
MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; UC = usual care; FSI = Fatigue Symptom Inventory; PSQI = Pittsburgh Sleep Quality Index; MDASI = M.D. Anderson Symptom Inventory.
Table 3.
Mean Symptom Reports by Random Assignment and Time Point for Each Measure Comprising the Pain Cluster
| MBSR(BC) |
UC |
|||||
|---|---|---|---|---|---|---|
| Cluster Pain | Mean | SD | n | Mean | SD | n |
| Quality of life (SF-36) | ||||||
| Baseline | 62.44 | 27.52 | 167 | 62.74 | 24.68 | 155 |
| Week 6 | 65.76 | 26.18 | 152 | 66.24 | 24.76 | 145 |
| Week 12 | 68.43 | 27.76 | 153 | 70.36 | 22.70 | 146 |
| Severity (BPI) | ||||||
| Baseline | 11.30 | 10.12 | 167 | 9.69 | 8.60 | 155 |
| Week 6 | 9.59 | 9.44 | 157 | 8.28 | 8.16 | 151 |
| Week 12 | 8.46 | 9.41 | 161 | 8.66 | 8.40 | 155 |
MBSR(BC) = Mindfulness-Based Stress Reduction for Breast Cancer; UC = usual care; SF-36 = Short-Form General Health Survey; BPI = Brief Pain Inventory.
Disclosures and Acknowledgments
The project described was supported by award number 1R01CA131080–01A2 from the National Cancer Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health. This study protocol was approved by the Institutional Review Boards at the University of South Florida and Moffitt Cancer Center to ensure the ethical treatment of participants. The authors have no conflicts to report.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors. Informed consent was obtained from all individual participants included in the study.
References
- 1.American Cancer Society. Cancer facts & figures 2016 2016. Available at: http://www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2016/index. Accessed July 5, 2016.
- 2.Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975-2008. 2011. Available at: http://seer.cancer.gov/archive/csr/1975_2008/. Accessed July 5, 2016.
- 3.American Cancer Society. What are the key statistics about breast cancer?. 2015. Available at: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-key-statistics. Accessed December 10, 2015.
- 4.National Cancer Institute. Facing forward: life after cancer treatment. 2014. Available at: http://www.cancer.gov/Publications/patient-education/facing-forward. Accessed June 5, 2015.
- 5.Lengacher CA, Reich RR, Post-White J, et al. Mindfulness based stress reduction in post-treatment breast cancer patients: an examination of symptoms and symptom clusters. J Behav Med 2012;35:86–94. [DOI] [PubMed] [Google Scholar]
- 6.Dodd MJ, Cho MH, Cooper BA, Miaskowski C. The effect of symptom clusters on functional status and quality of life in women with breast cancer. Eur J Oncol Nurs 2010; 14:101–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Langford DJ, Paul SM, Cooper B, et al. Comparison of subgroups of breast cancer patients on pain and co-occurring symptoms following chemotherapy. Support Care Cancer 2016;24:605–614. [DOI] [PubMed] [Google Scholar]
- 8.Sarenmalm EK, Browall M, Gaston-Johansson F. Symptom burden clusters: a challenge for targeted symptom management: a longitudinal study examining symptom burden clusters in breast cancer. J Pain Symptom Manage 2014;47: 731–741. [DOI] [PubMed] [Google Scholar]
- 9.National Cancer Institute. Family caregivers in cancer (PDQ): Patient version. Bethesda: PDQ Supportive and Palliative Care Editorial Board, 2015, 2015. [Google Scholar]
- 10.Berger AM, Visovsky C, Hertzog M, Holtz S, Loberiza FR Jr. Usual and worst symptom severity and interference with function in breast cancer survivors. J Support Oncol 2012;10:112–118. [DOI] [PubMed] [Google Scholar]
- 11.Reinertsen KV, Grenaker Alnaes GI, Landmark-Hoyvik H, et al. Fatigued breast cancer survivors and gene polymorphisms in the inflammatory pathway. Brain Behav Immun 2011;25:1376–1383. [DOI] [PubMed] [Google Scholar]
- 12.Hall DL, Mishel MH, Germino BB. Living with cancer-related uncertainty: associations with fatigue, insomnia, and affect in younger breast cancer survivors. Support Care Cancer 2014;22:2489–2495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Morin CM, Belleville G, Belanger L, et al. The Insomnia Severity Index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011;34:601–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fu OS, Crew KD, Jacobson JS, et al. Ethnicity and persistent symptom burden in breast cancer survivors. J Cancer Surv 2009;3:241–250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ho SY, Rohan KJ, Parent J, et al. A longitudinal study of depression, fatigue, and sleep disturbances as a symptom cluster in women with breast cancer. J Pain Symptom Manage 2015;49:707–715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Starkweather AR, Lyon DE, Elswich RK Jr, et al. A conceptual model of psychoneurological symptom cluster variation in women with breast cancer: bringing nursing research to personalized medicine. Curr Pharmacogenomics Person Med 2013;11:224–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dodd MJ, Miaskowski C, Paul SM. Symptom clusters and their effect on the functional status of patients with cancer. Oncol Nurs Forum 2001;28:465–470. [PubMed] [Google Scholar]
- 18.Roiland RA, Heidrich SM. Symptom clusters and quality of life in older adult breast cancer survivors. Oncol Nurs Forum 2011;38:672–680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Denieffe S, Cowman S, Gooney M. Symptoms, clusters and quality of life prior to surgery for breast cancer. J Clin Nurs 2014;23:2491–2502. [DOI] [PubMed] [Google Scholar]
- 20.Fiorentino L, Rissling M, Liu L, Ancoli-Israel S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: severity of the problem and treatment options. Drug Discov Today Dis Models 2011;8: 167–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Carlson LE, Garland SN. Impact of mindfulness-based stress reduction (MBSR) on sleep, mood, stress and fatigue symptoms in cancer outpatients. Int J Behav Med 2005;12: 278–285. [DOI] [PubMed] [Google Scholar]
- 22.Lengacher C, Johnson-Mallard V, Post-White J, et al. Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psychooncology 2009;18:1261–1272. [DOI] [PubMed] [Google Scholar]
- 23.National Center for Complementary and Integrative Health. Complementary, alternative, or integrative health: what’s in a name?. 2016. Available at: https://nccih.nih.gov/sites/nccam.nih.gov/files/CAM_Basics_Whats_In_A_Name_03-26-2015.pdf. Accessed July 5, 2016.
- 24.Henderson VP, Massion AO, Clemow L, et al. A randomized controlled trial of mindfulness-based stress reduction for women with early-stage breast cancer receiving radiotherapy. Integr Cancer Ther 2013;12:404–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moskowitz MC, Feuerstein M, Todd BL. Job stress and physical activity related to elevated symptom clusters in breast cancer survivors at work. J Occup Environ Med 2013;55:93–98. [DOI] [PubMed] [Google Scholar]
- 26.Wurtzen H, Dalton SO, Elsass P, et al. Mindfulness significantly reduces self-reported levels of anxiety and depression: results of a randomised controlled trial among 336 Danish women treated for stage I-III breast cancer. Eur J Cancer 2013;49:1365–1373. [DOI] [PubMed] [Google Scholar]
- 27.Cleeland CS, Mendoza TR, Wang XS, et al. Assessing symptom distress in cancer patients: the M.D. Anderson Symptom Inventory. Cancer 2000;89:1634–1646. [DOI] [PubMed] [Google Scholar]
- 28.Kabat-Zinn J, Lipworth L, Burney R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J Behav Med 1985;8:163–190. [DOI] [PubMed] [Google Scholar]
- 29.Kabat-Zinn J, Massion AO, Kristeller J, et al. Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. Am J Psychiatry 1992;149: 936–943. [DOI] [PubMed] [Google Scholar]
- 30.Speca M, Carlson LE, Goodey E, Angen M. A randomized, wait-list controlled clinical trial: the effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosom Med 2000;62:613–622. [DOI] [PubMed] [Google Scholar]
- 31.Vickberg SM. The Concerns about Recurrence Scale (CARS): a systematic measure of women’s fears about the possibility of breast cancer recurrence. Ann Behav Med 2003;25:16–24. [DOI] [PubMed] [Google Scholar]
- 32.Radloff L The CES-D scale: a self-report depression scale for researching the general population. Appl Psychol Meas 1977;1:385–401. [Google Scholar]
- 33.Yang L, Jia CX, Qin P. Reliability and validity of the Center for Epidemiologic Studies Depression Scale (CES-D) among suicide attempters and comparison residents in rural China. BMC Psychiatry 2015;15:76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Atkins R Validation of the center for epidemiologic studies depression scale in black single mothers. J Nurs Meas 2014;22:511–524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Spielberger C, Gorsuch R, Luschene R. Manual for the State-trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists, 1983. [Google Scholar]
- 36.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav 1983;24: 385–396. [PubMed] [Google Scholar]
- 37.Feldman G, Hayes A, Kumar S, Greeson J, Laurenceau JP. Mindfulness and emotion regulation: the development and initial validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). J Psychopathol Behav Assess 2007;29:177–190. [Google Scholar]
- 38.Mendoza TR, Zhao F, Cleeland CS, et al. The validity and utility of the M. D. Anderson Symptom Inventory in patients with breast cancer: evidence from the symptom outcomes and practice patterns data from the eastern cooperative oncology group. Clin Breast Cancer 2013;13: 325–334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Carpenter JS, Andrykowski MA. Psychometric evaluation of the Pittsburgh sleep quality Index. J Psychosom Res 1998;45:5–13. [DOI] [PubMed] [Google Scholar]
- 40.Hann DM, Denniston MM, Baker F. Measurement of fatigue in cancer patients: further validation of the Fatigue Symptom Inventory. Qual Life Res 2000;9:847–854. [DOI] [PubMed] [Google Scholar]
- 41.Keller S, Bann CM, Dodd SL, et al. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin J Pain 2004;20:309–318. [DOI] [PubMed] [Google Scholar]
- 42.Farias ST, Mungas D, Harvey DJ, et al. The measurement of everyday cognition (ECog): scale development and psychometric properties. Neuropsychology 2008;22: 531–544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 survey manual and interpretation guide. Boston: New England Medical Center, The Health Institute, 1993. [Google Scholar]
- 44.Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equation Model 1999;6: 1–55. [Google Scholar]
- 45.Steiger JH. Understanding the limitations of global fit assessment in structural equation modeling. Pers Individ Dif 2007;42:893–898. [Google Scholar]
- 46.Muthén LK, Muthén BO. Mplus user’s guide, 7th ed. Los Angeles: Muthén & Muthén, 1998–2003. [Google Scholar]
- 47.Lengacher CA, Reich RR, Paterson CL, et al. Examination of broad symptom improvement due to Mindfulness-Based Stress Reduction for Breast Cancer Survivors: a randomized controlled trial. J Clin Oncol 2016;34:2827–2834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rosenzweig S, Greeson JM, Reibel DK, et al. Mindfulness-based stress reduction for chronic pain conditions: variation in treatment outcomes and role of home meditation practice. J Psychosom Res 2010;68:29–36. [DOI] [PubMed] [Google Scholar]
- 49.McMillan SC, Tofthagen C, Morgan MA. Relationships among pain, sleep disturbances, and depressive symptoms in outpatients from a comprehensive cancer center. Oncol Nurs Forum 2008;35:603–611. [DOI] [PubMed] [Google Scholar]
- 50.Cheung WY, Le LW, Gagliese L, Zimmerman C. Age and gender differences in symptom intensity and symptom clusters among patients with metastatic cancer. Support Care Cancer 2011;19:417–423. [DOI] [PubMed] [Google Scholar]
- 51.Fan G, Hadi S, Chow E. Symptom clusters in patients with advanced-stage cancer referred for palliative radiation therapy in an outpatient setting. Support Cancer Ther 2007;4:157–162. [DOI] [PubMed] [Google Scholar]
- 52.Kirkova J, Aktas A, Walsh D, Rybicki L, Davis MP. Consistency of symptom clusters in advanced cancer. Am J Hosp Palliat Care 2010;27:342–346. [DOI] [PubMed] [Google Scholar]
- 53.Maliski SL, Kwan L, Elashoff D, et al. Symptom clusters related to treatment for prostate cancer. Oncol Nurs Forum 2008;35:786–793. [DOI] [PubMed] [Google Scholar]