

ABSTRACT
Background
Over-the-counter, natural product–based (nonvitamin, nonmineral) dietary supplement (NVNM DS) use is common in adults with rheumatoid arthritis (RA), a group at risk for drug-DS interactions, due to polypharmacy, but this use is underreported to health care providers. Recent dramatic changes in US sales of specific NVNM DS suggest that the prevalence and types of NVNM DS used in RA populations may also have shifted.
Objectives
A study was undertaken to identify current and past use of specific NVNM DS for RA disease treatment and to examine associations between use of NVNM DS, RA pharmaceuticals, and/or vitamin or mineral (VM) DS.
Methods
We developed a survey instrument to capture current and ever use of specific NVNM DS, VM DS, and RA pharmaceuticals, with 696 subjects self-reporting an RA diagnosis recruited online or in clinic for survey participation. Analyses were limited to 611 subjects reporting RA diagnosis after age 18 y and treatment with specific RA pharmaceuticals.
Results
Most participants reported DS use, with current usage prevalence 49.6% (n = 303), 83.5% (n = 510), or 87.6% (n = 535) for NVNM, VM, or any DS, respectively. While not having appeared in previous RA surveys, turmeric and ginger were among the top 3 NVNM DS in current use, along with fish oil/ω-3 (n–3) PUFA. Concurrent NVNM DS use was reported by 48.2% (n = 243) of participants currently using RA pharmaceuticals (n = 504) and was more common in those using disease-modifying antirheumatic drugs only (no biologics). Most methotrexate users (83%) reported concurrent folate supplementation, with one-third also using turmeric, which is notable because methotrexate and turmeric have been associated with hepatotoxicity.
Conclusion
Individuals with RA commonly use NVNM DS in combination with RA pharmaceuticals, including a previously undocumented but popular use of turmeric or ginger supplements with an unclear risk/benefit ratio.
Keywords: rheumatoid arthritis, dietary supplements, complementary and alternative medicine, turmeric, vitamins, herbals, natural products
Introduction
Natural product–derived, nonvitamin, nonmineral (NVNM) dietary supplements (DS), such as glucosamine or fish oil, are the most common complementary and alternative medicine modality used by the general population in the United States, with treatment of musculoskeletal complaints being the most common reason for their use (1). Although the prevalence of NVNM DS use by adults in the general population has remained constant at 18–19% over the past decade, the specific products used have not, as reflected both by sales data and reported patterns of use in national health surveys (2–5). For example, use of fish oil and probiotics by the general population has increased, whereas use of glucosamine and/or chondroitin sulfate (G&CS) has decreased (1).
National surveys have documented higher DS use in women, those taking prescription medicines, and those with chronic diseases (6, 7). Therefore, as summarized in a scoping review of the literature recently published by our research group, it is not surprising that NVNM DS use is even more common in adults with rheumatoid arthritis (RA) (31–60% prevalence), a chronic systemic autoimmune disorder disproportionately affecting women (77% of patients in RA registries) that is managed with intensive pharmacologic regimens (8–10). Although pharmacologic management of RA has advanced rapidly in recent years (11), studies indicate that incentives remain for patients with RA to incorporate DS into their treatment regimen, including dissatisfaction with current treatments and perceived benefits of the added treatment (4). Averse pharmacodynamic or pharmacokinetic interactions between NVNM DS and drugs are well documented (12–14); however, interactions between NVNM DS and RA pharmaceuticals have not specifically been studied. However, individuals with RA have a higher theoretical risk for adverse effects associated with NVNM DS due to their frequent use of multiple pharmaceuticals with known side effects (10), as well as associated systemic manifestations of the disease itself. Critically, because only a minority of patients with RA report NVNM DS use to their providers (9), any such untoward effects could be attributed to other causes and thus go unnoticed.
Given this apparently widespread but individually underreported use of NVNM DS in RA, data from population-based surveys identifying current patterns of specific NVNM DS use are of great relevance for clinical RA management. However, previously published studies, as summarized in our recent review of the literature (9), are limited in scope in terms of design and size (median, n = 153), with almost half having been published more than a decade ago. Thus, data reflecting current NVNM DS usage in RA are limited. For example, since 2010, only 3 of 7 reports are full publications (compared with abstracts) (9): a study detailing usage by African Americans in the southern United States (15) and 2 non-US studies (16, 17), only 1 of which included data on specific products used. Even in studies collecting information on specific products, inclusion of open-ended questions to capture products beyond those prespecified is uncommon; of 8 US studies reported since 1983 (9), only 1 published in 2004 (n = 95) appears to have incorporated this element of study design (18). In addition, although overall prevalence of NVNM DS use in RA appears similar across time (1980–2015) and geographical locations, averaging 47% (9), no study has directly compared specific product use between culturally and/or geographically distinct populations (e.g., between countries), and multiregional data from the United States are only available in abstract form (19). In addition, no studies have examined associations between use of NVNM DS and cohort characteristics, including concurrent use of specific RA pharmaceuticals (9).
Therefore, a comprehensive assessment to identify a full range of specific types of NVNVM DS used by individuals with RA was undertaken to include simultaneous assessment of usage patterns across the United States, including the western United States, an understudied region for which the most recent data, published over a decade ago (2004), were limited to 95 subjects (18). An additional primary aim of this study, given the potential for DS-drug interactions in a population with high polypharmacy use, was to examine associations between use of NVNM DS and prescribed RA pharmaceuticals, as well as over-the-counter vitamin or mineral DS (VM DS) recommended for use in RA by health care providers, for example, vitamin D to mitigate bone loss or folate to counter toxic effects of methotrexate (20, 21), a common first-line RA pharmaceutical (10). Associations between other cohort characteristics and patterns of DS use were also assessed.
Methods
Survey development and data management
A survey questionnaire was developed by the research team, which included a scientist diagnosed with RA, to capture detailed information related to past and present use of the following interventions for RA disease management: 1) specific NVNM DS, with inclusion of open-ended questions to capture a full range of products used; 2) specific VM DS, such as vitamin D, with potential roles in RA management (20, 21); and 3) specific RA pharmaceuticals recommended and commonly prescribed for RA (10). Because some natural products can be administered via culinary intake as well as ingestion of commercial DS (e.g., turmeric), to better capture the full usage spectrum for a particular natural product, limited information about dietary approaches used for RA management was also captured for dietary use of specific products and also, for general interest, the use of specific diets (e.g., paleo). After the first 100 responses were collected, the study team updated the survey to include line item queries for the most commonly reported NVNM supplements or dietary components (querying current, past, never, or unsure use) to simplify delivery and later analysis while retaining capture of “other” product information (current and/or past) that could be itemized for entry by each respondent (Supplemental Figure 1). At this time, opioid narcotics were also added to the list of RA medications specifically queried, as a question of general interest not included in any analysis. The survey was primarily completed by participants online using a custom link through REDCap (Research Electronic Data Capture) (22), a web-based platform also used for survey data management, with data from a limited number of hard-copy versions of the survey that were completed by participants (n = 22) added to the database by research personnel.
Recruitment and survey delivery
This study, which complies with the Declaration of Helsinki, was approved by the Institutional Review Board at the University of Arizona (IRB #1503767303). Participants were provided with information to allow for implied consent prior to beginning the survey, which was anonymous, with online access only allowing survey completion if the respondent first self-reported a diagnosis of RA, the sole criterion for survey completion (no exclusionary criteria). Initial recruitment efforts were geographically focused in southern Arizona and were limited to 1) local media coverage (newspaper, television, and radio with associated online content), 2) the distribution of advertising and/or hard-copy versions of the surveys to local rheumatology practices, and 3) the distribution of flyers within the community. A second phase of recruitment was added to broaden recruitment geographically using social media outlets (RA patient advocacy blogs and support groups, Facebook website and advertisements, and Twitter posts). No access to medical records was required for participation; therefore, to be included in subsequent data analyses, an RA diagnosis was further validated through self-report of current and/or prior use of specific RA pharmaceuticals (see Supplemental Figure 1), which are grouped and reported here as either traditional disease-modifying antirheumatic drugs (DMARDs) or biologics, including tofacitinib (biologics) (10), with those lacking this history excluded. In total, 786 surveys were collected over 20 months (January 2016–August 2017) (Figure 1), with n = 36 being completed by patients during visits to local rheumatology clinics (hard copies or online). Incomplete surveys, duplicate responses, and those reporting no RA diagnosis or age of diagnosis <18 years old, suggestive of possible juvenile idiopathic arthritis (previously known as juvenile rheumatoid arthritis) (23), were excluded from any analysis (Figure 1). Respondents had the choice of completing the survey in English or in Spanish; however, only 7 surveys were completed in Spanish, of which 4 were excluded, for reasons described above. In total, 90 surveys were excluded, with a final sample of 696 surveys from individuals with self-reported RA diagnosed at or after 18 years of age (Figure 1). From this sample, only surveys from individuals who also reported current and/or past use of specific DMARDs and/or biologics recommended by the American College of Rheumatology for RA “treatment to target” (10), consistent with a health provider–validated diagnosis of RA, were included in analyses associations between NVNM DS use and other cohort characteristics (n = 611).
FIGURE 1.
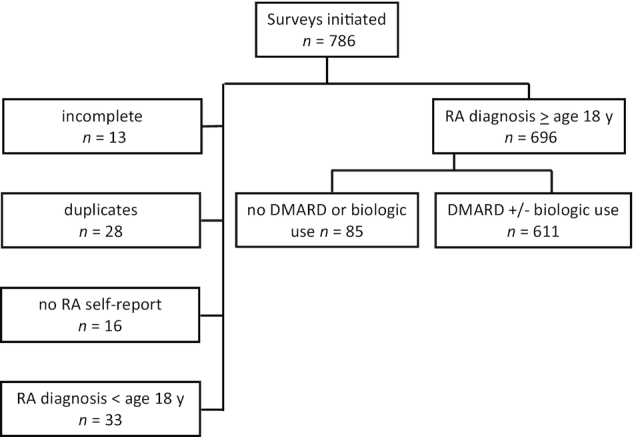
Survey schematic. Flowchart indicates survey data collected and exclusionary criteria applied to limit analyses to subjects with self-reported RA diagnosed ≥age 18 y and a history of RA pharmaceutical use. DMARD, disease-modifying antirheumatic drug; RA, rheumatoid arthritis.
Statistical analysis
Demographic data were assessed using descriptive statistics, mean ± SD for continuous measures, and percentages for categorical responses. In cross-sectional analyses of usage prevalence for treatment modalities (NVNM DS, VM DS, or dietary approaches) and specific products, “ever” use was defined as current or past usage, and “never” use included both never and “unsure” responses.
Geographical differences in ever use of treatment modalities or current use of specific DS and associations of current DS use and current RA medication were evaluated using Pearson χ2 test, with post hoc analysis using pairwise comparison and Bonferroni's correction. Associations between ever use of DS (VM or NVNM) and the variables of age, sex, ethnicity, RA disease duration, ever use of other DS, or ever use of biologics, a marker for a lack of response to first-line DMARDs and health care provider attempts to treat-to-target (10, 24), were computed using multiple logistic regression. Both univariate- and multivariate-adjusted models produced substantially similar results, with modest changes to coefficient estimates, confidence intervals, and P values. Only results from the covariate-adjusted analyses (ORs and 95% CIs) are reported here. For all analyses, type I error rate was controlled at 0.05. Results were computed using STATA 14.2 (StataCorp LLC).
Results
Participant characteristics
As would be expected based on RA patient registry data (8) and population-based surveys (25, 26), in a sample of 696 individuals with a self-report diagnosis of RA at ≥18 years of age, the majority were middle-aged non-Hispanic women, having a mean disease duration of 9.8 years (Table 1). Ever use of DMARDs or biologics, consistent with a health care provider diagnosis of RA, was reported by all but 12% of respondents (Table 2), with a lower prevalence of current usage. Ever use of anti-inflammatory and/or analgesic agents was also common (Table 2). Most participants resided in the United States, with disproportionate representation from the western United States and, more specifically, Arizona, consistent with planned recruitment goals and methods (Table 1). For all subsequent analyses, the sample was limited to those reporting ever use of RA pharmaceuticals (DMARDs and/or biologics), consistent with a provider-based diagnosis of RA (n = 611), the majority of whom (82.5%, n = 504) also reported current usage of DMARDs and/or biologics (Table 2).
TABLE 1.
Characteristics of participants with self-reported RA (n = 696)
| Characteristic | Value1 |
|---|---|
| Age, y | 52.5 ± 13.2 (52) |
| Age at diagnosis, y | 42.6 ± 12.8 (41) |
| Time since diagnosis, y | 9.8 ± 9.4 (6) |
| Sex, n (%) | |
| Female | 646 (92.8) |
| Male | 50 (7.2) |
| Ethnicity, n (%) | |
| Non-Hispanic | 613 (88.2) |
| Hispanic | 82 (11.8) |
| Not disclosed | 1 (<0.5) |
| Race, n (%) | |
| White | 607 (87.2) |
| Black or African American | 11 (1.6) |
| Asian | 7 (1.0) |
| American Indian or Alaska Native | 10 (1.4) |
| Native Hawaiian, other Pacific Islander | 1 (<0.5) |
| Other/mixed | 32 (4.6) |
| Not disclosed | 28 (4.0) |
| Geographic location | |
| United States, n (% of total) | 579 (83.2) |
| West, n (% of United States) | 281 (48.5) |
| Arizona, n (% of West) | 194 (69.0) |
| South, n (% of United States) | 138 (23.8) |
| Midwest, n (% of United States) | 98 (16.9) |
| Northeast, n (% of United States) | 52 (9.0) |
| Not disclosed, n (% of United States) | 10 (1.7) |
| Other countries, n (% of total) | 117 (16.8) |
| Commonwealth,2n (% of Other) | 80 (68.4) |
Values are means ± SDs (median) or number of observations (n) and percentages (%). All missing data <1% (n = 4 age or age at diagnosis; n = 1, ethnicity). RA, rheumatoid arthritis.
Australia, Canada, and United Kingdom.
TABLE 2.
RA pharmaceutical use by participants with self-reported RA (n = 696)1
| Pharmaceutical | Ever use | Current use |
|---|---|---|
| Any DMARDs and/or biologics | 611 (87.8) | 504 (72.4) |
| Any DMARDs | 594 (85.3) | 413 (59.3) |
| Methotrexate | 525 (75.4) | 292 (42.0) |
| Hydroxychloroquine | 368 (52.9) | 177 (25.4) |
| Sulfasalazine | 47 (6.8) | 30 (4.3) |
| Any biologics | 350 (50.3) | 250 (35.9) |
| Anti-inflammatory/analgesic | ||
| Steroids, oral | 506 (72.7) | 167 (24.0) |
| NSAIDs | 600 (86.2) | 358 (51.4) |
| Opioids2 | 265 (44.1) | 132 (22.0) |
Values are number of observations (n) and percentages (%). DMARDs, disease-modifying antirheumatic drugs; NSAIDs, nonsteroidal anti-inflammatory drugs; RA, rheumatoid arthritis.
Opioid use data only captured for n = 601.
Prevalence and patterns of NVNM DS use in RA
Ever or current NVNM DS usage was reported by at least half of participants with self-reported RA and history of DMARD and/or biologic use [62.8% (n = 384) and 49.6% (n = 303), respectively] (Figure 2A), with most current NVNM DS users reporting use of more than 1 product and 23.8% (n = 72) reporting concurrent use of ≥4 NVNM DS (Figure 2B). Fish oil/ω-3 PUFA DS were the most common NVNM DS reported for ever use [47.6% (n = 291)] (Figure 3A), followed by turmeric [43.5% (n = 266)], G&CS [29.6% (n = 181)], and ginger [25.5% (n = 156)]. However, patterns of current usage were different (Figure 3A); turmeric was the most common NVNM DS in current usage [30.3% (n = 185)], and current use of ginger [13.3% (n = 81)], a plant botanically and chemically related to turmeric (27), was more prevalent than G&CS [8.2% (n = 50)]. When examining associations between NVNM DS use and cohort characteristics, there were no geographic differences in the prevalence of ever usage of NVNM DS or specific NVNM DS with a high prevalence of use (Table 3), with the exception of ever use of ginger DS, which was more common outside of the United States. Ever use of NVNM DS was not associated with age, sex, or RA disease duration (Table 4) but was 1.9-fold more likely in non-Hispanics and was also more common in ever VM DS users.
FIGURE 2.

Use of DS or dietary approaches (individual component or specific dietary pattern) for RA management, as reported by participants with self-reported RA and a history of RA pharmaceutical use (n = 611). (A) Prevalence of use (ever or current) for NVNM DS, VM DS, any DS, or dietary approaches (DIET APPR), including individual dietary components or specific diets (n = 611). (B) Prevalence of concurrent use of multiple DS products among current users of NVNM DS (n = 303) or current users of VM DS (n = 535). DIET APPR, dietary approach; DS, dietary supplement; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
FIGURE 3.

Specific DS products used for RA management, as reported by participants with self-reported RA and a history of RA pharmaceutical use (n = 611). (A) Specific NVNM DS products used (ever or current). (B) Specific VM DS products used (ever or current). *Indicates data not available for certain products where past use was not recorded, precluding calculation of ever use. DS, dietary supplement; G&CS, glucosamine and/or chondroitin sulfate; MSM, methylsulfonylmethane; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
TABLE 3.
Prevalence of treatment modality or specific product use by geographic region for participants with self-reported RA and a history of RA pharmaceutical use (n = 611)1
| Modality or product | United States (n = 510) | Other countries (n = 101) | P value | Western United States (n = 248) | Other US regions (n = 262) | P value |
|---|---|---|---|---|---|---|
| Ever use | ||||||
| NVNM DS | 62.5 | 64.4 | 0.73 | 62.1 | 63.0 | 0.84 |
| VM DS | 89.4 | 88.1 | 0.51 | 86.7 | 92.0 | 0.052 |
| Dietary approach | 32.0 | 41.6 | 0.06 | 30.6 | 33.2 | 0.50 |
| Current use | ||||||
| Any turmeric2 | 34.1 | 32.7 | 0.78 | 33.9 | 34.4 | 0.91 |
| Turmeric DS | 30.0 | 31.7 | 0.74 | 30.2 | 29.8 | 0.90 |
| Fish oil/ω-3 PUFA DS | 27.8 | 29.7 | 0.70 | 29.4 | 26.3 | 0.43 |
| Ginger DS | 12.0 | 19.8 | 0.03 | 12.5 | 11.5 | 0.71 |
Values are percentages. DS, dietary supplement; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
Includes turmeric DS and/or dietary turmeric root/tea.
TABLE 4.
Association of ever DS use with characteristics of participants with self-reported RA and a history of RA pharmaceutical use (n = 606)1
| Ever NVNM DS use | Ever VM DS use | ||||
|---|---|---|---|---|---|
| Characteristic | N | Adjusted OR (95% CI) | P value | Adjusted OR (95% CI) | P value |
| Age | 606 | 1.00 (0.99–1.02) | 0.55 | 0.99 (0.97–1.01) | 0.37 |
| Time since RA | 606 | 1.00 (0.98–1.02) | 0.75 | 1.02 (0.98–1.05) | 0.36 |
| Sex | |||||
| Female | 564 | 1 (reference) | 1 (reference) | ||
| Male | 42 | 0.60 (0.31–1.16) | 0.13 | 0.89 (0.34–2.31) | 0.81 |
| Ethnicity | |||||
| Non-Hispanic | 533 | 1 (reference) | 1 (reference) | ||
| Hispanic | 73 | 0.54 (0.32–0.90) | 0.018 | 1.41 (0.60–3.32) | 0.43 |
| Ever RA biologic use | |||||
| User | 348 | 1 (reference) | 1 (reference) | ||
| Nonuser2 | 258 | 1.49 (1.04–2.14) | 0.03 | 0.70 (0.40–1.24) | 0.23 |
| Ever NVNM DS use | |||||
| User | 379 | — | 1 (reference) | ||
| Nonuser | 227 | — | 0.18 (0.10–0.33) | <0.0001 | |
| Ever VM DS use | |||||
| User | 542 | 1 (reference) | — | ||
| Nonuser | 64 | 0.18 (0.10–0.32) | <0.0001 | — | |
Participants missing answers for any of the covariates (age, time since diagnosis, sex, ethnicity, or biologic use, a marker of insufficient response to first-line disease-modifying antirheumatic drugs (DMARDs) and attempts to treat to target) were excluded from analysis (n = 5 excluded, <1%). Values are number of observations (n) or adjusted OR and 95% CI. DS, dietary supplements; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
Only DMARDs use (ever).
Prevalence and patterns of VM DS use in RA
Rates of ever or current VM DS usage were also high [89.2% (n = 545) and 83.5% (n = 510), respectively] (Figure 2A). Most current VM DS users reported use of more than 1 VM DS (Figure 2B), with 44.3% (n = 226) reporting concurrent use of ≥4 VM DS. Specific VM DS products most commonly used, in descending order of prevalence for both ever or current use (Figure 3B), were vitamin D, folate, multivitamins, and calcium. When examining associations between VM DS use and cohort characteristics, there were no geographical differences in ever VM DS usage (Table 3). Ever use of VM DS was strongly associated with ever NVNM DS use (OR: 5.4; P < 0.0001) (Table 4) but not age, sex, ethnicity, or RA disease duration (Table 3). Among current DS users (n = 535), 52.0% reported concurrent use of VM and NVNM DS (n = 278).
Prevalence and patterns of dietary approaches used in RA
Ever or current use of dietary approaches for RA management (Figure 2) was reported by a minority of respondents [33.6% (n = 205) or 29.1% (n = 178), respectively]. Although dietary approaches tended to be more common in non-US countries, this trend was not statistically significant (Table 3). Individual dietary components most commonly reported (ever or current use) were green tea (15.9% current, n = 97), turmeric (13.9% current, n = 85), and coconut oil (11.3% current, n = 69) (Supplemental Table 1). When turmeric use in any form was considered (culinary and/or DS), the prevalence of “any” turmeric usage rose only slightly, as compared with prevalence of turmeric DS use alone, with no differences in usage between countries or within the United States (Table 3). Therefore, for subsequent analyses, turmeric usage was limited to an assessment of turmeric DS. Specific diets most commonly reported (ever or current use) were gluten-free (12.6% current, n = 77), anti-inflammatory (8.8% current, n = 54), and paleo diets (5.9%, n = 36) (Supplemental Table 1).
Associations between DS and RA pharmaceuticals usage
When examining associations between NVNM DS and RA pharmaceutical usage, ever use of NVNM DS (Table 4) was 1.5-fold more common in those who had never been treated with biologics. Similarly, concurrent use of NVNM DS (Table 5) with RA pharmaceuticals was more frequent in those currently using DMARD-only treatment (no biologics). Current usage of each of the 3 most commonly reported NVNM DS (turmeric, fish oil/ω-3 PUFA, ginger) (Table 5) was also higher in individuals currently only taking DMARDs (no biologics), although these differences were only statistically significant for turmeric. Among methotrexate users, concurrent use of methotrexate and turmeric DS was reported by 29.1% (n = 85 of 292). In individuals reporting prior but no current DMARD or biologic use (Table 5, neither) current usage of NVNM DS or specific NVNM DS products was similar to the DMARD-only group and thus higher than the biologic group; however, these trends were not statistically significant. Unlike NVNM DS, the prevalence of ever VM DS use had no association with ever biologic use (Table 4). However, current VM DS use was more common in those currently using DMARDs and/or biologics as compared with those using neither (Table 5). Concurrent folate use was reported by most methotrexate users (83%, n = 243 of 292), consistent with RA treatment guidelines (21).
TABLE 5.
Concurrent use of DS with RA pharmaceuticals in participants with self-reported RA and a history of RA pharmaceutical use (n = 611)1
| Current RA pharmaceutical use, % | ||||
|---|---|---|---|---|
| Current DS use | DMARDs only (n = 254) | Biologics2 (n = 250) | Neither3 (n = 107) | P value4 |
| NVNM DS | 53.5 | 42.8 | 56.1 | 0.0475 |
| Turmeric DS | 34.6 | 24.8 | 32.7 | 0.0495 |
| Fish oil/ω-3 PUFA DS | 31.5 | 24 | 29.9 | >0.05 |
| Ginger DS | 14.2 | 10 | 18.7 | >0.05 |
| VM DS | 84.6 | 88 | 70.1 | <0.0026 |
Values are percentages. DMARDs, disease-modifying antirheumatic drugs; DS, dietary supplement; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
With or without concurrent DMARDs use ( n = 91 individuals on biologics only).
Reported past, but not current, DMARDs and/or biologics use.
Pairwise comparisons using Bonferroni's correction.
Biologic compared with DMARDs only.
Neither compared with DMARDs only and neither compared with biologics.
Discussion
In studies published over the past 4 decades, NVNM DS use in RA exceeded that of the general adult population more than 2-fold, with marine oils and G&CS being the most commonly used products worldwide and in the United States (9). In the current study, although prevalence remained high and use of marine oils and G&CS was still common, there were also notable differences. Most striking was the identification of turmeric as the most common NVNM DS currently used worldwide and in the United States (30% prevalence) and the increasingly prevalent use of ginger (13%), a plant botanically related to turmeric (27, 28). In contrast, neither turmeric nor ginger appeared in prior RA studies (9), with the exception of 2 US studies published more than a decade ago documenting infrequent (<5%) use (18, 29). This increased prevalence mirrors temporal shifts in US sales, as turmeric and ginger currently hold third and sixth place among top-selling botanical DS sales in the United States, after a decade of exponential or doubling of sales, respectively (2, 3, 5).
However, compelling scientific evidence of efficacy does not appear to be driving these changes in NVNM DS use in RA. Only 4 small clinical studies (n = 86 total subjects treated) using products of variable (and undocumented) composition and doses for short-term treatment have been published and provide some evidence for turmeric DS tolerability and efficacy in ameliorating joint symptoms in RA, only 2 of which were randomized, double blinded, and placebo controlled (30–33). For ginger, we are aware of only a single short-term clinical trial (n = 35 treated) testing a ginger product of uncharacterized composition, demonstrating benefits in reducing RA joint symptoms (34). Because botanical products, unlike drugs, are chemically complex, a lack of characterization of product content in these botanical clinical trials is a particular concern, a limitation compounded by the relative lack of US federal oversight of the content of botanical DS sold (35–37). Of the other 2 top NVNM DS documented here, more data are available for fish oil/ω-3 PUFU in RA, with evidence of moderate quality demonstrating efficacy in reducing RA joint symptoms and improving risk factors for cardiovascular disease, a systemic manifestation of RA (38–40). In contrast, a placebo-controlled study investigating glucosamine in RA did not demonstrate efficacy (41).
Certain unique elements of our study design could have also contributed to differences in specific NVNM DS identified and their prevalence compared with previous studies (9). Two such elements and particular strengths of this study were its large size, relative to prior studies, and the inclusion of open-ended queries to ensure capture of a complete range of DS products used. Additionally, recruitment of participants outside of the setting of rheumatology specialty clinics, uncommon in prior studies (9), may also have captured a wider population with variable access to care. An additional strength of this study was its simultaneous assessment of NVNM usage patterns across geographic areas in the United States, including the western United States, which had not been surveyed in almost 2 decades, and Arizona, a population never previously assessed (9). It was not clear when systematically reviewing prior published studies whether geographic differences in product usage between studies were due to cultural, temporal, or other factors (9); however, in the current study, patterns of NVNM DS use were similar across US regions and when compared with other countries, with the notable exception of ginger DS use, which was more prevalent in non US-countries. These findings suggest that prior unique patterns of NVNM DS use in noncontemporaneous studies could have been more reflective of temporal rather than geographic or cultural trends. At the same time, it must be noted that the current study, whose recruitment methods were focused on US populations, was underpowered to assess US compared with non-US NVNM DS use. The fact that ginger DS use was still found to be significantly higher in non-US countries suggests that global differences still exist.
A limitation of this study is its reliance on a self-selected cohort, which could have overrepresented individuals with a particular interest in NVNM DS. However, the similar prevalence of NVNM DS usage reported here across geographic regions compared with prior RA studies, including those assessing RA registry data (9), suggests that self-selection was likely not a major limiting factor. A second limitation of the study design was its reliance on a self-report of RA not verified through medical records or direct assessment of RA criteria in study participants (23). However, elimination of individuals with likely juvenile idiopathic arthritis (previously known as juvenile RA) (23) and those lacking a detailed history of treatment with specific RA pharmaceuticals (DMARDs and/or biologics), as recommended for RA treatment by the American College of Rheumatology (10), likely limited inclusion to those diagnosed with RA by health care providers. A lack of validation of the DS survey method by physical inspection of actual NVNM DS products used, analogous to methodology used for NHANES (42), is a limitation of this study, as was the lack of inclusion of queries related to dosing, duration of use, or information about the source of recommendations influencing NVNM DS product use.
A unique strength of this study, compared with earlier reports (9), was its analysis of associations between use of NVNM DS and cohort characteristics. Although not queried here, because of prior evidence that individuals with RA infrequently report NVNM DS use to providers (9), such population-based data may provide insights relevant to patient safety. The preponderance of middle-aged women in this study is reflective of RA patient populations in general (e.g., 64–86% women in RA patient registries, with average age 50–68 y) (8); however, underrepresentation of men (7%) was a study limitation, such that lower reported ever use of NVNM DS by men was not statistically significant. Hispanics were also underrepresented (25, 26); however, ever NVNM DS use by Hispanics was still found to be significantly lower than in non-Hispanics.
Because biologics are recommended in RA when first-line DMARD treatments are insufficient to meet treatment goals (10, 24), biologic use (ever, never, or current) was a key variable in analyses assessing associations between cohort characteristics and NVNM DS use. It was thus notable that subjects reporting ever or current use of biologics were less likely to report ever or concurrent use of NVNM DS. Because patients with RA, on or off biologics, often do not reach target treatment goals (10, 24), it is possible that individuals on first-line DMARDs turn to NVNM DS more frequently in lieu of biologics. In this regard, a limitation of this study was the lack of information gathered related to systemic manifestations of RA or other comorbidities that could have influenced NVNM DS choices.
From a safety standpoint, it is notable that concurrent use of NVNM DS with RA pharmaceuticals was reported by almost half of the participants, including concurrent use of 3 or more NVNM DS by more than one-third. Because adverse pharmacodynamics or pharmacokinetic interactions between DS and pharmaceuticals are not uncommon (12–14) and NVNM DS content is variable and minimally regulated (35–37), frequent use of any NVNM DS, including turmeric, the most common, should provide a cautionary note for health care providers when assessing clinical responses in RA populations. Focusing on turmeric as an example, as is true for many NVNM DS frequently used for RA (9), although preclinical evidence supports RA treatment efficacy (43, 44), clinical evidence of both efficacy and safety is scant for RA (30–33). Notably, although published turmeric clinical trials in non-RA populations suggest a 5% risk of liver injury that is likely idiosyncratic (45), a recent report of turmeric DS-induced autoimmune hepatitis (45) and emerging international reports of turmeric DS-related liver damage (46) suggest that caution should be exercised when monitoring turmeric DS use in those at higher risk for autoimmune diseases and/or possible hepatotoxic drug-DS interactions. Indeed, because methotrexate induces liver enzyme elevations in one-third of users (47) and one-third of methotrexate users in this current study reported concurrent turmeric DS use, it is readily apparent that a potential role for turmeric in contributing to hepatocellular damage in RA methotrexate users could be obscured if turmeric use was not disclosed by the patient and/or considered by the physician.
Ever use of NVNM DS was more common in those also reporting ever use of VM DS, with use of 3 or more VM DS reported by the majority of current VM DS users. Vitamin D, postulated to play a role in RA pathogenesis when deficient and known to mitigate musculoskeletal side effects associated with RA and/or its treatment (48–50), was the most commonly used VM DS product. However, given reports of a higher prevalence of vitamin D deficiency in RA populations (49), it is notable that only 63% of respondents reported current vitamin D use. Similarly, concurrent use of methotrexate with folate (including leucovorin), the second most commonly used VM DS, although common and consistent with current guidelines aimed at mitigating methotrexate gastrointestinal side effects and liver toxicity (21, 47), was reported by only 83% of methotrexate users, possibly reflecting noncompliance.
As with all treatment plans, open communication between patients and providers about multimodal approaches to RA management is likely to enhance clinical outcomes related to safety and efficacy, even when high-quality data are lacking. Because NVNM DS use is frequently not reported by individual patients with RA to health care professionals (9), the population-based data presented here may help direct these conversations while also potentially identifying relevant NVNM DS for further study to address both safety and efficacy in RA populations.
Supplementary Material
Acknowledgments
We thank Lena Feng and Rachel Groff for their contributions to initial survey design and revision, Anthony German-Martinez for his efforts toward in-clinic recruitment, and the community rheumatologists in Tucson, Arizona, who were willing to participate and support our study, most especially, Dr. Shannon Howe.
The authors’ responsibilities were as follows: JLF and ALH: research design; MBS, LLH, and JLK: conducted research; MBS, DB, and JLF: data and statistical analyses; MBS, JLF: writing of paper; and JLF: primary responsibility for final content. All authors have read and approved the final manuscript.
Notes
Source of support: This research was supported by the National Center for Complementary and Integrative Health (NCCIH) at the NIH (R34AT007837). Views expressed here are solely the responsibility of the authors and do not necessarily represent those of the NIH or NCCIH.
Author disclosures: The authors report no conflicts of interest.
Supplemental Table 1 and survey tool (Supplemental Figure 1) are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at http://jn.nutrition.org.
Abbreviations used: DMARDs, disease-modifying antirheumatic drugs; DS, dietary supplement; G&CS, glucosamine and/or chondroitin sulfate; NVNM, nonvitamin, nonmineral; RA, rheumatoid arthritis; VM, vitamin or mineral.
Contributor Information
Meghan B Skiba, Department of Health Promotion Sciences, University of Arizona, Tucson, AZ, USA; Department of Medicine, University of Arizona, Tucson, AZ, USA.
Laura L Hopkins, Department of Medicine, University of Arizona, Tucson, AZ, USA; Department of Nutritional Sciences, University of Arizona, Tucson, AZ, USA.
Allison L Hopkins, Department of Anthropology, Texas A&M University, College Station, TX, USA.
Dean Billheimer, Department of Epidemiology and Biostatistics, University of Arizona, Tucson, AZ, USA.
Janet L Funk, Department of Medicine, University of Arizona, Tucson, AZ, USA; Department of Nutritional Sciences, University of Arizona, Tucson, AZ, USA.
References
- 1. Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002–2012. National Health Statistics Reports. 2015;79:1–16. [PMC free article] [PubMed] [Google Scholar]
- 2. Cavaliere C, Rea P, Lynch ME, Blumenthal M. Herbal supplement sales experience slight increase in 2008. HerbalGram. 2009;82:58–61. [Google Scholar]
- 3. Linstrom A, Ooyen C, Lynch ME, Blumenthal M. Herb supplement sales increase 5.5% in 2012: herbal supplement sales rise for the 9th consecutive year; turmeric sales jump 40% in natural channel. HerbalGram. 2013;99:60–5. [Google Scholar]
- 4. Rose G. Why do patients with rheumatoid arthritis use complementary therapies?. Musculoskelet Care. 2006;4:101–15. [DOI] [PubMed] [Google Scholar]
- 5. Smith T, Gillespie M, Eckl V, Knepper J, Reynolds CM. Herbal supplement sales in US increase by 9.4% in 2018. HerbalGram. 2019;123:62–73. [Google Scholar]
- 6. Wilson PB. Dietary supplementation is more prevalent among adults with arthritis in the United States population. Complement Ther Med. 2016;29:152–7. [DOI] [PubMed] [Google Scholar]
- 7. Falci L, Shi Z, Greenlee H. Multiple chronic conditions and use of complementary and alternative medicine among us adults: results from the 2012 National Health Interview Survey. Prev Chronic Dis. 2016;13:E61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Curtis JR, Jain A, Askling J, Bridges SL Jr, Carmona L, Dixon W, Finckh A, Hyrich K, Greenberg JD, Kremer J et al. A comparison of patient characteristics and outcomes in selected European and U.S. rheumatoid arthritis registries. Semin Arthritis Rheum. 2010;40:2–14..e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. DeSalvo JC, Skiba MB, Howe CL, Haiber KE, Funk JL. Natural product dietary supplement use by individuals with rheumatoid arthritis: a scoping review. Arthritis Care Res. 2019;71:787–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Singh JA, Saag KG, Bridges SL Jr, Akl EA, Bannuru RR, Sullivan MC, Vaysbrot E, McNaughton C, Osani M, Shmerling RH et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68:1–26. [DOI] [PubMed] [Google Scholar]
- 11. Kumar LD, Karthik R, Gayathri N, Sivasudha T. Advancement in contemporary diagnostic and therapeutic approaches for rheumatoid arthritis. Biomed Pharmacother. 2016;79:52–61. [DOI] [PubMed] [Google Scholar]
- 12. Asher GN, Corbett AH, Hawke RL. Common herbal dietary supplement-drug interactions. Am Fam Physician. 2017;96:101–7. [PubMed] [Google Scholar]
- 13. Gardiner P, Phillips R, Shaughnessy AF. Herbal and dietary supplement–drug interactions in patients with chronic illnesses. Am Fam Physician. 2008;77:73–8. [PubMed] [Google Scholar]
- 14. Izzo AA, Ernst E. Interactions between herbal medicines and prescribed drugs: an updated systematic review. Drugs. 2009;69:1777–98. [DOI] [PubMed] [Google Scholar]
- 15. Tamhane A, McGwin G Jr, Redden DT, Hughes LB, Brown EE, Westfall AO, Conn DL, Jonas BL, Smith EA, Brasington RD et al. Complementary and alternative medicine use in African Americans with rheumatoid arthritis. Arthritis Care Res. 2014;66:180–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Mohd Noor N, Jenm DH, Hussein H, Mohd Isa L, Shahril NS. Influence of diet in inducing flares and use of dietary supplement in patients with rheumatoid arthritis. Int J Rheum Dis. 2012;15:145. [Google Scholar]
- 17. Alaaeddine N, Okais J, Ballane L, Baddoura RM. Use of complementary and alternative therapy among patients with rheumatoid arthritis and osteoarthritis. J Clin Nurs. 2012;21:3198–204. [DOI] [PubMed] [Google Scholar]
- 18. Herman CJ, Allen P, Hunt WC, Prasad A, Brady TJ. Use of complementary therapies among primary care clinic patients with arthritis. Prev Chronic Dis. 2004;1:A12. [PMC free article] [PubMed] [Google Scholar]
- 19. Pepmueller PH JR, Sharma A, Grant S, Saunders KC. Use and long term use of complementary and alternative medicine in rheumatoid arthritis patients [abstract]. Arthritis Rheum. 2012;64:S164–5. [Google Scholar]
- 20. Heidari B, Hajian-Tilaki K, Babaei M. Vitamin D deficiency and rheumatoid arthritis: epidemiological, immunological, clinical and therapeutic aspects. Mediterr J Rheumatol. 2019;30:94–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Singh JA. Folic acid supplementation for rheumatoid arthritis patients on methotrexate: the good gets better. Cochrane Database Syst Rev. 2013;7:ED000063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO III, Birnbaum NS, Burmester GR, Bykerk VP, Cohen MD et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69:1580–8. [DOI] [PubMed] [Google Scholar]
- 24. van Vollenhoven R. Treat-to-target in rheumatoid arthritis—are we there yet?. Nat Rev Rheumatol. 2019;15:180–6. [DOI] [PubMed] [Google Scholar]
- 25. US census data (2018). Washington (DC): United States Census Bureau; [Internet][accessed 2020 Jul 21]. Available from: https://www.census.gov/quickfacts/fact/table/US/RHI725218. [Google Scholar]
- 26. Helmick CG, Felson DT, Lawrence RC, Gabriel S, Hirsch R, Kwoh CK, Liang MH, Kremers HM, Mayes MD, Merkel PA et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008;58:15–25. [DOI] [PubMed] [Google Scholar]
- 27. Ramirez-Ahumada Mdel C, Timmermann BN, Gang DR. Biosynthesis of curcuminoids and gingerols in turmeric (Curcuma longa) and ginger (Zingiber officinale): identification of curcuminoid synthase and hydroxycinnamoyl-CoA thioesterases. Phytochemistry. 2006;67:2017–29. [DOI] [PubMed] [Google Scholar]
- 28. Funk JL, Frye JB, Oyarzo JN, Timmermann BN. Comparative effects of two gingerol-containing Zingiber officinale extracts on experimental rheumatoid arthritis. J Nat Prod. 2009;72:403–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Callahan LF, Wiley-Exley EK, Mielenz TJ, Xiao C, Currey SS, Sleath BL, Sloane PD, DeVellis RF, Brady TJ, Sniezek J. Use of complementary and alternative medicine among patients with arthritis. Prev Chronic Dis. 2009;6:A44. [PMC free article] [PubMed] [Google Scholar]
- 30. Amalraj A, Varma K, Jacob J, Divya C, Kunnumakkara AB, Stohs SJ, Gopi S. A novel highly bioavailable curcumin formulation improves symptoms and diagnostic indicators in rheumatoid arthritis patients: a randomized, double-blind, placebo-controlled, two-dose, three-arm, and parallel-group study. J Med Food. 2017;20:1022–30. [DOI] [PubMed] [Google Scholar]
- 31. Chandran B, Goel A. A randomized, pilot study to assess the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytother Res. 2012;26:1719–25. [DOI] [PubMed] [Google Scholar]
- 32. Deodhar SD, Sethi R, Srimal RC. Preliminary study on antirheumatic activity of curcumin (diferuloyl methane). Indian J Med Res. 1980;71:632–4. [PubMed] [Google Scholar]
- 33. Javadi M, Khadem Haghighian H, Goodarzy S, Abbasi M, Nassiri-Asl M. Effect of curcumin nanomicelle on the clinical symptoms of patients with rheumatoid arthritis: a randomized, double-blind, controlled trial. Int J Rheum Dis. 2019;22:1857–62. [DOI] [PubMed] [Google Scholar]
- 34. Aryaeian N, Shahram F, Mahmoudi M, Tavakoli H, Yousefi B, Arablou T, Jafari Karegar S. The effect of ginger supplementation on some immunity and inflammation intermediate genes expression in patients with active rheumatoid arthritis. Gene. 2019;698:179–85. [DOI] [PubMed] [Google Scholar]
- 35. Skiba MB, Luis PB, Alfarara C, Billheimer D, Schneider C, Funk JL. Curcuminoid content and safety-related markers of quality of turmeric dietary supplements sold in an urban retail marketplace in the United States. Mol Nutr Food Res[epub ahead of print 29 May 2018]. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Job KM, Kiang TK, Constance JE, Sherwin CM, Enioutina EY. Herbal medicines: challenges in the modern world. Part 4. Canada and United States. Expert Rev Clin Pharmacol. 2016;9:1597–609. [DOI] [PubMed] [Google Scholar]
- 37. Sax JK. Dietary supplements are not all safe and not all food: how the low cost of dietary supplements preys on the consumer. Am J Law Med. 2015;41:374–94. [DOI] [PubMed] [Google Scholar]
- 38. Gioxari A, Kaliora AC, Marantidou F, Panagiotakos DP. Intake of ω-3 polyunsaturated fatty acids in patients with rheumatoid arthritis: a systematic review and meta-analysis. Nutrition. 2018;45:114–24.e4. [DOI] [PubMed] [Google Scholar]
- 39. James M, Proudman S, Cleland L. Fish oil and rheumatoid arthritis: past, present and future. Proc Nutr Soc. 2010;69:316–23. [DOI] [PubMed] [Google Scholar]
- 40. Senftleber NK, Nielsen SM, Andersen JR, Bliddal H, Tarp S, Lauritzen L, Furst DE, Suarez-Almazor ME, Lyddiatt A, Christensen R. Marine oil supplements for arthritis pain: a systematic review and meta-analysis of randomized trials. Nutrients. 2017;9:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Nakamura H, Masuko K, Yudoh K, Kato T, Kamada T, Kawahara T. Effects of glucosamine administration on patients with rheumatoid arthritis. Rheumatol Int. 2007;27:213–8. [DOI] [PubMed] [Google Scholar]
- 42. Dwyer J, Picciano MF, Raiten DJ. Collection of food and dietary supplement intake data: what we eat in America—NHANES. J Nutr. 2003;133:590s–600s. [DOI] [PubMed] [Google Scholar]
- 43. Funk JL, Oyarzo JN, Frye JB, Chen G, Lantz RC, Jolad SD, Solyom AM, Timmermann BN. Turmeric extracts containing curcuminoids prevent experimental rheumatoid arthritis. J Nat Prod. 2006;69:351–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Funk JL, Frye JB, Oyarzo JN, Kuscuoglu N, Wilson J, McCaffrey G, Stafford G, Chen G, Lantz RC, Jolad SD et al. Efficacy and mechanism of action of turmeric supplements in the treatment of experimental arthritis. Arthritis Rheum. 2006;54:3452–64. [DOI] [PubMed] [Google Scholar]
- 45. Lukefahr AL, McEvoy S, Alfafara C, Funk JL. Drug-induced autoimmune hepatitis associated with turmeric dietary supplement use. BMJ Case Reports. 2018;2018:bcr–2018-224611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Luber RP, Rentsch C, Lontos S, Pope JD, Aung AK, Schneider HG, Kemp W, Roberts SK, Majeed A. Turmeric induced liver injury: a report of two cases. Case Rep Hepatol. 2019;2019:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Visser K, Katchamart W, Loza E, Martinez-Lopez JA, Salliot C, Trudeau J, Bombardier C, Carmona L, van der Heijde D, Bijlsma JW et al. Multinational evidence-based recommendations for the use of methotrexate in rheumatic disorders with a focus on rheumatoid arthritis: integrating systematic literature research and expert opinion of a broad international panel of rheumatologists in the 3E Initiative. Ann Rheum Dis. 2009;68:1086–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Buckley LM, Leib ES, Cartularo KS, Vacek PM, Cooper SM. Effects of low dose methotrexate on the bone mineral density of patients with rheumatoid arthritis. J Rheumatol. 1997;24:1489–94. [PubMed] [Google Scholar]
- 49. Vojinovic J, Tincani A, Sulli A, Soldano S, Andreoli L, Dall'Ara F, Ionescu R, Pasalic KS, Balcune I, Ferraz-Amaro I et al. European multicentre pilot survey to assess vitamin D status in rheumatoid arthritis patients and early development of a new Patient Reported Outcome questionnaire (D-PRO). Autoimmun Rev. 2017;16:548–54. [DOI] [PubMed] [Google Scholar]
- 50. Peng J, Gong Y, Zhang Y, Xiao Z, Zeng Q, Chen S. Bone mineral density in patients with rheumatoid arthritis and 4-year follow-up results. J Clin Rheumatol. 2016;22:71–4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.