

Abstract
The complexity of cancer chemotherapy requires pharmacists be familiar with the complicated regimens and highly toxic agents used. This column reviews various issues related to preparation, dispensing, and administration of antineoplastic therapy, and the agents, both commercially available and investigational, used to treat malignant diseases. Questions or suggestions for topics should be addressed to Dominic A. Solimando, Jr., President, Oncology Pharmacy Services, Inc., 4201 Wilson Blvd #110–545, Arlington, VA 22203, e-mail: [email protected]; or J. Aubrey Waddell, Professor, University of Tennessee College of Pharmacy; Oncology Pharmacist, Pharmacy Department, Blount Memorial Hospital, 907 E. Lamar Alexander Parkway, Maryville, TN 37804, e-mail: [email protected].

INDICATIONS
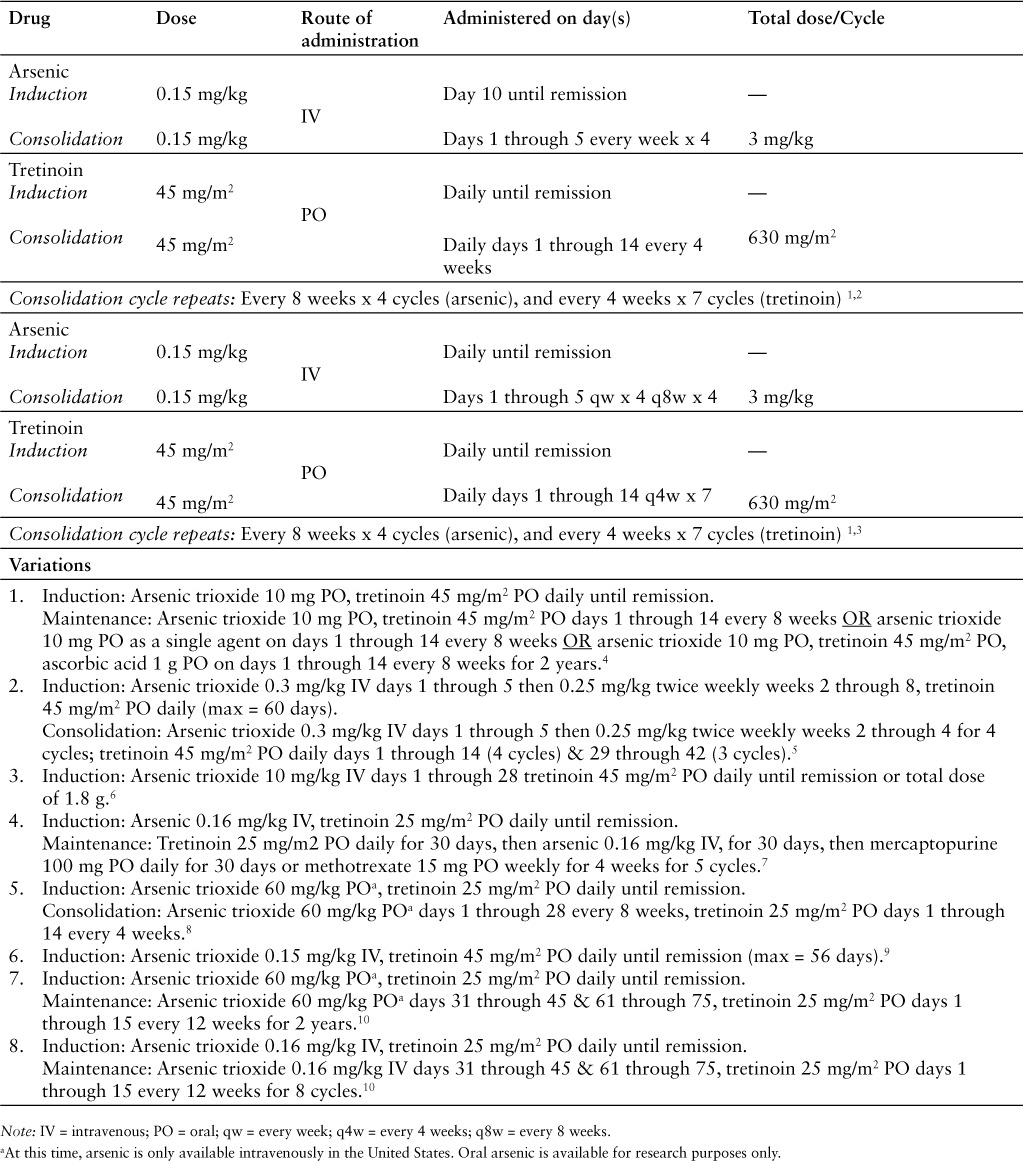
Arsenic trioxide and tretinoin (AsO/ATRA) has been studied for the treatment of acute promyelocytic leukemia (APL) (Table 1).1–10 It is the preferred induction regimen for newly diagnosed patients with APL who have low-risk disease (white blood cell count [WBC] ≤10,000/mcL), and it is the recommended induction regimen for patients with high-risk disease (WBC >10,000/mcL) who cannot tolerate anthracyclines. 11 Patients who receive this regimen for induction will also receive arsenic and tretinoin for maintenance and, in some regimens, consolidation therapy. Additionally, AsO/ATRA is recommended for APL patients who relapse and have no prior exposure to arsenic or who relapse at least 6 months after completing an arsenic-containing regimen.11
Table 1.
Arsenic trioxide and tretinoin regimen
DRUG PREPARATION
Follow institutional policies for preparation of hazardous medications when preparing arsenic and dispensing tretinoin.
- Arsenic
- Use arsenic solution 1 mg/mL.
- Dilute in 100 to 250 mL of 0.9% sodium chloride (NS) or 5% dextrose solution (D5W) for infusion.
- Tretinoin
- Tretinoin is available as 10 mg capsules.
- Store at 20° to 25°C (68° to 77°F).
DRUG ADMINISTRATION
- Arsenic trioxide
- Arsenic is infused intravenously over 1 to 3 hours.
- Many protocols require an electrocardiogram (EKG) at baseline and at least weekly thereafter. If the QTc interval exceeds 500 msec, the infusion is delayed until it is less than 460 msec.
- The manufacturer recommends not administering the drug if the12:
- (1) QTc is greater than 500 msec.
- (2) Serum potassium is less than or equal to 4 mEq/mL.
- (3) Serum magnesium is less than or equal to 1.8 mg/dL.
SUPPORTIVE CARE
- A. APL Differentiation Syndrome: The rate of differentiation syndrome in patients treated with arsenic and tretinoin ranges from 3% to 40%.1,5,6,8,10 Signs and symptoms of differentiation syndrome include dyspnea, unexplained fever, weight gain, peripheral edema, unexplained hypotension, acute renal failure or congestive heart failure, interstitial pulmonary infiltrates, and pleuropericardial effusion. Reported treatments of differentiation syndrome include:
- Dexamethasone 10 mg intravenous (IV) every 12 hours until the resolution of symptoms and for a minimum of 3 days. Temporarily discontinue tretinoin, arsenic, or both. When symptoms improve, resume treatment at 50% of the previous dose for 7 days and then resume at full dose.3
- Dexamethasone 10 mg IV every 12 hours for 5 days followed by a 2-week taper. 11
Some arsenic and tretinoin regimens give prophylactic steroids to prevent differentiation syndrome. 1,3 If differentiation syndrome occurs in this setting, guidelines recommend discontinuing the prophylactic steroids in favor of dexamethasone 10 mg IV every 12 hours.11
B. Acute and Delayed Emesis Prophylaxis: The AsO/ATRA regimen is predicted to cause acute emesis in 30% to 90% of patients.13–16 However, in the studies reviewed, severe nausea and vomiting occurred in only 1% of patients.1 Although the accepted model for predicting emetogenicity would consider the AsO/ATRA regimen to be moderately emetogenic,13–16 the actual incidence and severity of nausea and vomiting reported in the trials reviewed suggest it may be only mildly emetogenic, particularly on days when arsenic trioxide is not given.1–3 While a serotonin antagonist and steroid combination is recommended for moderately emetogenic regimens,14–16 for most patients a combination antiemetic regimen may not be required. Use of a serotonin antagonist should be avoided when giving arsenic trioxide due to the risk of QT wave prolongation with both agents; a dopamine antagonist may be more appropriate.
- For most patients, prophylactic antiemetic therapy is not required. If a patient does require prophylactic therapy, one of the following regimens is recommended:
- Prochlorperazine 10 mg orally (PO), ±diphenhydramine 25 to 50 mg PO if needed, given 30 minutes before AsO.
- Metoclopramide 0.5 to 2 mg/kg PO, ±diphenhydramine 25 to 50 mg PO if needed, given 30 minutes before AsO.
- Promethazine 25 to 50 mg PO, ±diphenhydramine 25 to 50 mg PO if needed, given 30 minutes before AsO.
- C. Breakthrough Nausea and Vomiting13–16: Patients should receive a prescription for an antiemetic to treat breakthrough nausea. One of the following regimens is recommended:
- Metoclopramide 0.5 to 2 mg/kg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed.
- Prochlorperazine 10 mg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 6 hours if needed.
- Prochlorperazine 25 mg rectally every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
- Promethazine 25 to 50 mg PO every 4 to 6 hours if needed, ±diphenhydramine 25 to 50 mg PO every 4 to 6 hours if needed.
Patients who do experience significant nausea or vomiting with one of these regimens should receive an agent from a different pharmacologic category.13–16
D. Diarrhea: Diarrhea is usually mild to moderate, responding to conventional therapy. Occasionally, the problem can be severe or dose limiting.
- Patients who experience diarrhea while receiving arsenic and tretinoin should receive an antidiarrheal agent. The standard recommendation is loperamide 4 mg PO at the onset of diarrhea, followed by 2 mg PO every after each unformed stool, or as often as every 2 hours for 24 hours.17 Patients should be counseled to18:
- Monitor bowel movements.
- Treat grade 1 or 2 diarrhea (increase of less than 7 stools per day or nocturnal stools) with loperamide and oral re-hydration.
- Immediately seek advice from their physician, pharmacist, or nurse for persistent (≥24 hours) grade 1 or 2 diarrhea, or grade 3 diarrhea (increase of ≥7 stools per day or incontinence or symptoms of dehydration).
Patients who have diarrhea while receiving arsenic should have their electrolytes closely monitored.
MAJOR TOXICITIES
Most of the toxicities listed below are presented according to their degree of severity. Higher grades represent more severe toxicities. Although there are several grading systems for cancer chemotherapy toxicities, all are similar. One of the frequently used systems is the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf). Oncologists generally do not adjust doses or change therapy for grade 1 or 2 toxicities but make, or consider, dosage reductions or therapy changes for grade 3 or 4 toxicities. Incidence values are rounded to the nearest whole percent unless incidence was less than or equal to 0.5%.
A. Cardiovascular: QT prolongation 16%,3 atrial arrhythmia (grade 3 or 4) 4%.1
B. Dermatologic: Rash (grade 3 or 4) 1%.1
C. Gastrointestinal: Gastrointestinal 4%,3 nausea (grade 3 or 4) 1%.1
D. Hematologic: Neutropenia (grade 3 or 4) 46%,3 thrombocytopenia (grade 3 or 4) 59%.3
E. Hepatic: Liver dysfunction (grade 3 or 4) 63%. 3
F. Neurologic: Headache (grade 3 or 4) 6%.1
H. Miscellaneous: Differentiation syndrome 18%.1,
PRETREATMENT LABORATORY STUDIES NEEDED
- A. Baseline
- Aspartate aminotransferase/alanine aminotransferase (AST/ALT)
- Total bilirubin
- Serum creatinine
- Complete blood count (CBC) with differential
- Coagulation studies: prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen, D-dimer
- Serum electrolytes: potassium, magnesium, calcium
- Electrocardiogram (ECG)
- B. Frequency of Laboratory Testing During Induction
- C. Recommended Pretreatment Values: The minimally acceptable values to receive full-dose therapy in the protocols reviewed were:
DOSAGE MODIFICATIONS
- B. Liver Function
- Arsenic:
- Serum bilirubin, AST, or ALT greater than 5 times the upper limit of normal, discontinue arsenic and/or tretinoin. Resume at 50% of previous dose once studies are less than 4 times the upper limit of normal, then resume full dosage. If hepatoxicity recurs, arsenic and/or tretinoin should be discontinued.3
- No information available. The drug should be used cautiously in patients with hepatic dysfunction.12
- Tretinoin:
- Serum bilirubin, AST, or ALT greater than 5 times the upper limit of normal, discontinue arsenic and/or tretinoin. Resume at 50% of previous dose once studies are less than 4 times the upper limit of normal, then resume full dosage. If hepatoxicity recurs, arsenic and/or tretinoin should be discontinued. 3
- No information available.19
Footnotes
*Dr. Damery is a clinical pharmacist at the University of Kansas Hospital, Kansas City, Kansas. At the time this article was written, she was an Oncology Pharmacy Resident (PGY2) at the National Institutes of Health, Bethesda, Maryland.
REFERENCES
- 1.Ravandi F, Estey E, Jones D et al. Effective treatment of acute promyelocytic leukemia with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab ozogamicin. J Clin Oncol. 2009;27(4):504–510. doi: 10.1200/JCO.2008.18.6130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Estey E, Garcia-Manero G, Ferrajoli A et al. Use of all-trans retinoic acid plus arsenic trioxide as an alternative to chemotherapy in untreated acute promyelocytic leukemia. Blood. 2006;107(9):3469–3473. doi: 10.1182/blood-2005-10-4006. [DOI] [PubMed] [Google Scholar]
- 3.Lo-Coco F, Avvisati G, Vignetti M et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013;369(2):111–121. doi: 10.1056/NEJMoa1300874. [DOI] [PubMed] [Google Scholar]
- 4.Au WY, Kumana CR, Lee HK et al. Oral arsenic trioxide-based maintenance regimens for first complete remission of acute promyelocytic leukemia: A 10-year follow-up study. Blood. 2011;118(25):6535–6543. doi: 10.1182/blood-2011-05-354530. [DOI] [PubMed] [Google Scholar]
- 5.Burnett AK, Russell NH, Hills RK et al. Arsenic trioxide and all-trans retinoic acid treatment for acute promyelocytic leukaemia in all risk groups (AML17): Results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2015;16(13):1295–1305. doi: 10.1016/S1470-2045(15)00193-X. [DOI] [PubMed] [Google Scholar]
- 6.Dai CW, Zhang GS, Shen JK et al. Use of all-trans retinoic acid in combination with arsenic trioxide for remission induction in patients with newly diagnosed acute promyelocytic leukemia and for consolidation/maintenance in CR patients. Acta Haematol. 2009;121(1):1–8. doi: 10.1159/000204472. [DOI] [PubMed] [Google Scholar]
- 7.Shen ZX, Shi ZZ, Fang J et al. All-trans retinoic acid/As2O3 combination yields a high quality remission and survival in newly diagnosed acute promyelocytic leukemia. Proc Natl Acad Sci USA. 2004;101(15):5328–5335. doi: 10.1073/pnas.0400053101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhu HH, Huang XJ. Oral arsenic and retinoic acid for non-high-risk acute promyelocytic leukemia. N Engl J Med. 2014;371(23):2239–2241. doi: 10.1056/NEJMc1412035. [DOI] [PubMed] [Google Scholar]
- 9.Raffoux E, Rousselot P, Poupon J et al. Combined treatment with arsenic trioxide and all-trans-retinoic acid in patients with relapsed acute promyelocytic leukemia. J Clin Oncol. 2003;21(12):2326–2334. doi: 10.1200/JCO.2003.01.149. [DOI] [PubMed] [Google Scholar]
- 10.Zhu HH, Wu DP, Jin J et al. Oral tetra-arsenic tetra-sulfide formula versus intravenous arsenic trioxide as first-line treatment of acute promyelocytic leukemia: A multicenter randomized controlled trial. J Clin Oncol. 2013;31(33):4215–4221. doi: 10.1200/JCO.2013.48.8312. [DOI] [PubMed] [Google Scholar]
- 11.National Comprehensive Cancer Network NCCN Clinical Practice Guidelines—Acute Myeloid Leukemia. V.2016.1. https://www.nccn.org/professionals/physician_gls/pdf/aml.pdf. Accessed June 8, 2016. [DOI] [PubMed]
- 12.Trisenox [prescribing information] Frazer, PA: Cephalon, Inc.; 2015. [Google Scholar]
- 13.Hesketh PJ, Kris MG, Grunberg SM et al. Proposal for classifying the acute emetogenicity of cancer chemotherapy. J Clin Oncol. 1997;15(1):103–109. doi: 10.1200/JCO.1997.15.1.103. [DOI] [PubMed] [Google Scholar]
- 14.National Comprehensive Cancer Network NCCN Clinical Practice Guidelines—Antiemesis. V.2.2016. http://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf. Accessed June 19, 2016.
- 15.Basch E, Prestrud AA, Hesketh PJ et al. Antiemetics: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2011;29(31):4189–4198. doi: 10.1200/JCO.2010.34.4614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Multinational Association for Supportive Care in Cancer/European Society for Medical Oncology Antiemetic guidelines. 2016.V.1.2. http://www.mascc.org/assets/Guidelines-Tools/mascc_antiemetic_guidelines_english_2016_v.1.2.pdf. Accessed June 19, 2016.
- 17.Maroun JA, Anthony LB, Blais N et al. Prevention and management of chemotherapy-induced diarrhea in patients with colorectal cancer: A consensus statement by the Canadian Working Group on chemotherapy-induced diarrhea. Curr Oncol. 2007;14(1):13–20. doi: 10.3747/co.2007.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Benson AB, Ajani JA, Catalano RB et al. Recommended guidelines for the treatment of cancer treatment-induced diarrhea. J Clin Oncol. 2004;22(14):2918–2926. doi: 10.1200/JCO.2004.04.132. [DOI] [PubMed] [Google Scholar]
- 19.Tretinoin, [prescribing information] Sellersville, PA: Teva Pharmaceuticals USA; 2010. [Google Scholar]