

Abstract
Objective
Time spent in sedentary behavior has been associated with worse inflammation and cardio-metabolic biomarkers in various populations. However, the association between time spent in sedentary behavior and biomarkers remains unknown in intermittent claudication patients. The aim of the current study was to analyze the relationship between sedentary behavior and inflammatory and cardio-metabolic biomarkers in patients with symptomatic peripheral artery disease (PAD).
Methods
The sample included 297 patients with intermittent claudication. Sedentary behavior was assessed using a step activity monitor. Biomarkers of inflammation, oxidative stress, lipid profile, insulin resistance and endogenous fibrinolysis were assessed. Demographic data, body mass index, physical activity status, measures of severity of PAD (ankle brachial index, peak walking time and ischemic window) also were obtained.
Results
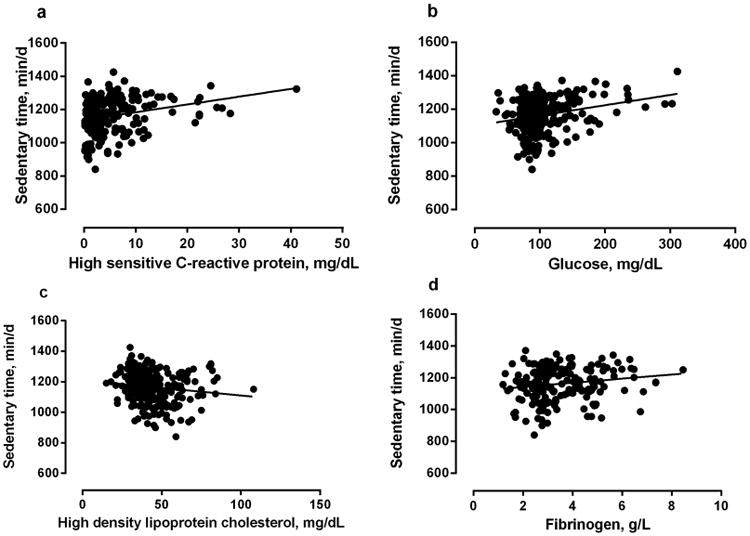
Time spent in sedentary behavior was related with high sensitive C-reactive protein (HsCRP) (b = 0.187 P=.005), glucose (b = 0.238, P<.001), fibrinogen (b = 0.167, P=.017), plasminogen activator inhibitor-1 activity (b = 0.143, P=.036) and high density lipoprotein cholesterol (HDL-C) (b = -0.133, P=.029). After adjustment for sex, age, physical activity status, body mass index and severity of PAD, sedentary behavior remained related with HsCRP (b = 0.170, P=.015), glucose (b = 0.178, P=.004), fibrinogen (b = 0.189, P=.010) and HDL-C (b = -0.128, P=.032).
Conclusion
Time spent in sedentary activities was associated with worse inflammatory and cardio-metabolic profile in intermittent claudication patients.
Introduction
Intermittent claudication, a prevalent symptom of peripheral artery disease (PAD) impairs walking capacity1 and reduces patients' quality of life2. PAD patients have elevated cardiovascular mortality rates3, which may be associated with their worse inflammatory, fibrinolytic, lipid and glucose profiles4.
Physical inactivity is one factor that may negatively impact vascular biomarkers in patients with PAD5. More recently, sedentary behavior has emerged as an important cardio-metabolic risk factor in the general population6-8, as greater time spent in sedentary activities is associated with type 2 diabetes, fatal and nonfatal cardiovascular disease, and all-cause mortality6-8. Sedentary behavior, which is distinct from physical inactivity, includes activities that are completed in a sitting or reclining posture, and activities consisting of low intensity characterized by energy expenditures ≤ 1.5 METs10, 11. In contrast, physical inactivity is defined by performing an insufficient amount of moderate-to-vigorous physical activity (i.e., not meeting specified physical activity guidelines)9, 10. Therefore, sedentary behavior and physical inactivity are different, as it is possible for an individual to accumulate large amounts of both moderate-to-vigorous physical activity and sedentary behavior in the course of a day11.
From this standpoint, previous studies have shown that greater time spent in sedentary behavior is associated with higher levels of inflammatory markers, lipids, glucose, insulin resistance and endogenous fibrinolysis, regardless of physical activity level12-14. However, sedentary behavior has not been examined in patients with PAD, who are likely to present high levels of sedentary behavior due to walking impairment observed in symptomatic patients15. Thus, the aim of the current study was to analyze the relationship between sedentary behavior and inflammatory and cardio-metabolic biomarkers in patients with symptomatic PAD.
Methods
Recruitment and Patients
Patients with Fontaine Stage II PAD16 were evaluated at the Clinical Research Center at the University of Oklahoma Health Sciences Center (HSC). Patients arrived fasted, but were permitted to take their usual medications. Patients were recruited by referrals from the HSC vascular clinics, as well as by newspaper advertisements for possible enrollment into an exercise study17, 18. The procedures of this study were approved by the Institutional Review Board at the University of Oklahoma HSC. Written informed consent was obtained from each patient prior to participation.
Patients performed an initial progressive, graded treadmill exercise test to determine study eligibility. Patients were included in the study if they met the following criteria: (a) graded treadmill test limited by intermittent claudication, (b) an ankle brachial index (ABI) ≤ 0.90 at rest19, or an ABI ≤ 0.73 after exercise20. Patients were excluded if they met any of the following criteria: (a) inability to obtain an ABI measure due to non-compressible vessels (ABI ≥ 1.40), (b) asymptomatic PAD determined from the medical history and verified during the graded treadmill test, and (c) exercise tolerance limited by factors other than claudication symptoms (e.g. clinically significant electrocardiographic changes during exercise indicative of myocardial ischemia, dyspnea, poorly controlled blood pressure), and (d) failure to complete the test procedures within three weeks. The total of 440 patients were deemed eligible for the study, and a total of 143 patients were excluded (110 screen failures and 33 who were non-compliant with testing). Thus, the final analysis consists of data from 297 patients.
Outcomes
Biomarkers
Blood Sampling
Blood was drawn by venipuncture from an antecubital vein, collected in vacutainers, and distributed in 0.5 ml aliquots. The samples were stored at -80°C, and were subsequently batched for analysis in duplicate in our laboratory at the Reynolds Oklahoma Center on Aging.
Plasma Lipoprotein Lipids, Glucose, and Insulin
Blood samples were drawn into chilled EDTA (1 mg/dl of blood) containing tubes after an overnight fast. Blood was analyzed for fasting lipids, glucose, and insulin levels as part of automated chemistry batteries, as detailed previously21. Total cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-C) were measured by standardized enzymatic procedure. Low-density lipoprotein cholesterol (LDL-C) was estimated by the Friedewald formula, and non-HDL-C was calculated as total cholesterol minus HDL-C22, 23.
High Sensitivity C-Reative Protein (HsCRP)
Concentration of HsCRP was quantified from 300 μl of sera using a high-sensitivity Near Infrared Particles Immunoassay. The SYNCHRON LX-20 (Beckman-Coulter; California, USA), a commercially available device, was used to perform the assay. Prior to performing each assay, the SYNCHRON system was calibrated, and a calibration curve was established24.
Oxidized LDL-C and Soluble vascular cell adhesion molecule (sVACAM-1)
Plasma oxidized LDL and sVCAM-1 were measured by immunoassay (Mercodia, Uppsala, Sweden and R&D Systems, Minneapolis, Minnesota) according to the manufacturer's protocol. For oxidized LDL, average intraassay precision is 5% and interassay precision is 8.7%. For sVCAM-1, average interassay precision is 3.9%.
Fribinogen and Endogenous Fibrinolysis
Fibrinogen was assayed in citrated plasma by a modified Clauss assay method. Endogenous fibrinolytic activity was quantified in all patients by measurements of serum Tissue plasminogen activator activity and Plasminogen activator inhibitor-1 activity (PAI-1). The antigen level of tPA was measured with an enzyme-linked immunoadsorbent assay (ELISA). Activity levels of tPA and PAI-1 were assayed by using an amidolytic method21. All assays were performed in duplicate, and interassay variability was determined to be <5%, as previously described25.
Predictors
Sedentary behavior
Sedentary behavior was assessed using a step activity monitor (StepWatch3™, Ortho innovations, Inc., Oklahoma City, OK) as previously described15. It was programmed by placing the unit on a USB docking station connected to a computer with StepWatch3™ Analysis Software. Physical activity was measured during seven consecutive days in which patients were instructed to wear the monitor during waking hours and to remove it before retiring to bed. The step activity monitor was attached to the right ankle above the lateral malleolus using elastic Velcro straps, and continuously recorded the number of steps taken on a minute-to-minute basis. The step activity monitor quantifies ambulatory stride rate and time of ambulatory activity and inactivity, and characterizes short-duration bursts of activity as well as sustained endurance. Sedentary behavior was considered the total time of inactivity per day (min/d), defined as the number of minutes in which zero strides were taken, included sleeping time.
Covariates
Physical Activity Status
The Johnson Space Center (JSC) physical activity scale 26 was used to assess the activity level of the participants over the preceding month. This 8-point Likert scale consists of the following score choices: 0 = avoid physical activities whenever possible, 1 = light physical activities done occasionally, 2 = moderate physical activities done regularly for less than 1 hour per week, 3 = moderate physical activities done regularly for more than 1 hour per week, 4 = heavy physical activities done regularly for less than 30 minutes per week, 5 = heavy physical activities done regularly between 30 and 60 minutes per week, 6 = heavy physical activities done regularly between 1 and 3 hours per week, and 7 = heavy physical activities done regularly for more than 3 hours per week. Patients were asked to select the appropriate score (0 to 7) which best described their general level of physical activity for the previous month. The JSC physical activity scale was previously used for PAD patients27.
Medical history and anthropometry
Demographic information, height, weight, body mass index, claudication history, physical examination and comorbid conditions (hypertension, diabetes, dyslipidemia, and heart disease) were assessed at the beginning of the study by a study physician. Hypertension was defined as systolic BP ≥ 140 mmHg or diastolic ≥ 90 mmHg, or use of anti-hypertensive medication. Diabetes was defined as fasting blood glucose ≥126 mg/dl, or use of hypoglycemic medication. Dyslipidemia was defined as triglycerides ≥ 150 mg/dL, LDL-C ≥ 160 mg/dL, total cholesterol ≥ 200 mg/dL or HDL-C ≤ 40 mg/dL (men) and ≤ 50 mg/dL (women), or use of lipid lowering medication. CAD was defined as a history of myocardial infarction or surgical procedures, or use of anti-angina medication.
ABI and ischemic window
ABI was obtained after 10 minutes of supine rest by measuring the ankle and brachial systolic blood pressure using Doppler technique in the brachial artery and both posterior tibial and dorsalis pedis arteries. The higher of the two arterial pressures from each leg was recorded, and the leg yielding the lower ABI was used for the analyses, as previously described28. After completion of a graded treadmill test, ankle and brachial systolic blood pressures were measured at 1, 3, 5, and 7 minutes during supine rest after exercise. Systolic ankle blood pressure was recorded during recovery from the graded treadmill test until baseline values were obtained. The time course of the reduction in ankle systolic blood pressure after treadmill exercise from the resting baseline value was quantified by calculating the area under the curve. Because the ischemic window is a function of both PAD severity and the amount of exercise performed, the ischemic window was normalized per meter walked29.
Claudication measurements
Graded treadmill test was used to assess claudication measurements. Patients performed a progressive graded cardiopulmonary treadmill test until maximal claudication pain, as previously described for PAD patients30. The test started at 2 mph with 0% grade and the workload was increased 2% every 2 minutes. All patients were familiarized with the test protocol before the experiments. The claudication onset time was defined as the walking time in which the patient first experienced pain in the legs, and the peak walking time was defined as the walking time in which the patients could not continue walking due the pain in the legs. Using these procedures, the test-retest intra-class reliability coefficients are r=0.89 for claudication onset time and r=0.93 for peak walking time31.
Statistical Analysis
All statistical analyses were performed using Statistical Package for the Social Sciences software – SPSS/PASW version 20 (IBM Corp, New York, USA). Continuous variables were summarized as mean and standard deviation, whereas categorical variables were summarized as relative frequency.
Unadjusted and adjusted analyses were performed by linear regression to analyze the relationship between sedentary behavior and biomarkers (HsCRP, insulin, glucose, HOMA-IR, oxidized LDL-C, sVCAM-1, triglyceride, cholesterol, HDL-C, LDL-C, plasma fibrinogen, t-PA activity and PAI-1 activity). In both analyses, each biomarker was included in a separate regression analysis. In multiple linear regressions, the relationship between sedentary behavior and cardio-metabolic biomarkers were adjusted in the Model 1 for confounders described previously in the literature6, 12-14, such as sex, age, body mass index, physical activity status. In the Model 2, adjustments were made to analyze the impact of disease severity in the relationship. Therefore, Model 2 consisted of adjusting for Model 1 variables plus severity of PAD (peak walking time, ABI and ischemic window). Residual analysis was performed, homoscedasticity was analyzed by graphical analysis (scatterplot) and adherence to the normal distribution was tested using the Kolmogorov-Smirnov test. Statistical significance was set at P<.05.
Results
Table I shows the clinical characteristics of patients, while the table II is shown the inflammatory and cardio-metabolic biomarkers of the patients included in the study.
Table I.
Characteristics of the intermittent claudication patients included in the study (n=297).
| Variables | Values |
|---|---|
| Mean ± Standard deviation | |
| Age, y | 65.2 ± 10.1 |
| Body mass index, kg/m2 | 29.4 ± 6.1 |
| Ankle brachial index | 0.71 ± 0.23 |
| Claudication onset time, s | 215 ± 182 |
| Peak walking time, s | 421 ± 280 |
| Ischemic window, mmHg/min/m | -0.58 ± 1.04 |
| Physical Activity Scale (activity score) | 1.5 ± 1.1 |
| Sedentary time, min/d | 1165 ± 104 |
| Frequency | |
| Sex, % male | 50.2 |
| Current smoking, % yes | 35.7 |
| Obesity, % yes | 44.4 |
| Diabetes mellitus, % yes | 42.8 |
| Hypertension, % yes | 87.3 |
| Dyslipidemia, % yes | 89.3 |
| Coronary artery disease, % yes | 35.0 |
Table II.
Biomarkers of the intermittent claudication patients included in the study.
| Biomarkers | Values |
|---|---|
| C-reactive protein, mg/dL (n=234) | 6.1 ± 11.3 |
| Insulin, mU/mL (n=213) | 14.4 ± 16.9 |
| Glucose, mg/dL (n=293) | 104.6 ± 39.4 |
| HOMA-IR (n=213) | 2.93 ± 4.92 |
| Soluble vascular cell adhesion molecule-1, ng/ml (n-=191) | 754.5 ± 285.7 |
| Oxidized low density lipoprotein, U/L (n=191) | 70.2 ± 25.1 |
| Triglyceride, mg/dL (n=292) | 157.6 ± 206.7 |
| Cholesterol, mg/dL (n=292) | 176.3 ± 40.6 |
| High density lipoprotein cholesterol, mg/dL (n=291) | 44.6 ± 14.0 |
| Low density lipoprotein cholesterol, mg/dL (n=281) | 102.7 ± 36.7 |
| Fibrinogen, g/L (n=220) | 3.4 ± 1.3 |
| Tissue plasminogen activator activity, IU/mL (n=217) | 0.65 ± 1.81 |
| Plasminogen activator inhibitor-1 activity, AU/mL (n=220) | 17.5 ± 20.0 |
The crude and adjusted relationships between sedentary behavior and biomarkers are shown in Table III. More time spent in sedentary behavior was positively correlated with higher levels of HsCRP, glucose, fibrinogen, and PAI-1 activity, and was negatively correlated with HDL-C (P<.05).
Table III.
Crude and adjusted analyses of the relationship between sedentary behavior and inflammatory and cardio-metabolic biomarkers in intermittent claudication patients.
| Dependent variables | Models | β (SE) | b | r | r2 | P |
|---|---|---|---|---|---|---|
| Inflammation | ||||||
| Crude | 0.020 (0.007) | 0.187 | 0.187 | 0.035 | .005 | |
| High sensitive C-reactive protein, mg/dL | Model 1 | 0.021 (0.007) | 0.196 | 0.235 | 0.055 | .004 |
| Model 2 | 0.018 (0.007) | 0.170 | 0.277 | 0.077 | .015 | |
| Diabetes measures | ||||||
| Crude | 0.092 (0.023) | 0.238 | 0.238 | 0.057 | <.001 | |
| Glucose, mg/dL | Model 1 | 0.080 (0.023) | 0.206 | 0.316 | 0.100 | .004 |
| Model 2 | 0.069 (0.024) | 0.178 | 0.340 | 0.115 | .001 | |
| Crude | 0.006 (0.011) | 0.042 | 0.042 | 0.002 | .556 | |
| Insulin, μU/mL | Model 1 | -0.003 (0.011) | 0.023 | 0.371 | 0.137 | .790 |
| Model 2 | -0.003 (0.011) | -0.019 | 0.408 | 0.167 | .790 | |
| Crude | 0.006 (0.003) | 0.123 | 0.123 | 0.015 | .080 | |
| HOMA-IR | Model 1 | 0.003 (0.003) | 0.057 | 0.357 | 0.127 | .424 |
| Model 2 | 0.003 (0.003) | 0.054 | 0.390 | 0.152 | .457 | |
| Oxidative stress | ||||||
| Crude | 0.102 (0.197) | 0.038 | 0.038 | 0.001 | .606 | |
| Soluble vascular cell adhesion molecule 1, ng/ml | Model 1 | 0.139 (0.202) | 0.053 | 0.191 | 0.037 | .493 |
| Model 2 | 0.124 (0.209) | 0.047 | 0.255 | 0.051 | .554 | |
| Crude | 0.011 (0.017) | 0.047 | 0.047 | 0.002 | .523 | |
| Oxidized low density lipoprotein, U/L | Model 1 | 0.006 (0.018) | 0.027 | 0.190 | 0.036 | .732 |
| Model 2 | 0.007 (0.019) | 0.031 | 0.211 | 0.044 | .704 | |
| Lipids | ||||||
| Crude | 0.136 (0.075) | 0.110 | 0.110 | 0.012 | .070 | |
| Triglyceride, mg/dL | Model 1 | 0.111 (0.076) | 0.089 | 0.255 | 0.065 | .146 |
| Model 2 | 0.097 (0.079) | 0.078 | 0.263 | 0.069 | .218 | |
| Crude | 0.007 (0.023) | 0.019 | 0.019 | 0.001 | .749 | |
| Cholesterol, mg/dL | Model 1 | 0.008 (0.024) | 0.021 | 0.229 | 0.053 | .729 |
| Model 2 | 0.004 (0.024) | 0.010 | 0.243 | 0.059 | .875 | |
| Crude | -0.018 (0.008) | -0.133 | 0.133 | 0.018 | .029 | |
| High density lipoprotein cholesterol, mg/dL | Model 1 | -0.019 (0.008) | -0.145 | 0.394 | 0.155 | .013 |
| Model 2 | -0.017 (0.008) | -0.128 | 0.403 | 0.162 | .032 | |
| Crude | -0.003 (0.022) | -0.007 | 0.007 | 0.001 | .904 | |
| Low density lipoprotein cholesterol, mg/dL | Model 1 | 0.004 (0.023) | 0.011 | 0.170 | 0.029 | .859 |
| Model 2 | -0.002 (0.024) | -0.005 | 0.188 | 0.036 | .939 | |
| Coagulation | ||||||
| Crude | 0.002 (0.001) | 0.161 | 0.161 | 0.026 | .017 | |
| Fibrinogen, g/L | Model 1 | 0.002 (0.001) | 0.199 | 0.282 | 0.080 | .006 |
| Model 2 | 0.002 (0.001) | 0.189 | 0.313 | 0.098 | .010 | |
| Crude | 0.001 (0.001) | 0.030 | 0.030 | 0.001 | .663 | |
| Tissue plasminogen activator activity, IU/mL | Model 1 | 0.001 (0.001) | 0.043 | 0.144 | 0.021 | .559 |
| Model 2 | 0.001 (0.001) | 0.042 | 0.174 | 0.030 | .578 | |
| Crude | 0.027 (0.013) | 0.143 | 0.143 | 0.02 | .036 | |
| Plasminogen activator inhibitor-1 activity, AU/mL | Model 1 | 0.007 (0.013) | 0.040 | 0.395 | 0.156 | .559 |
| Model 2 | 0.008 (0.013) | 0.041 | 0.408 | 0.166 | .562 | |
β (SE) regression coefficient (standard error), b standardized beta coefficients, r - multiple correlation coefficient for each model. r2 - variance for each model. Model 1 adjusted for sex, age, physical activity status, body mass index. Model 2 adjusted for Model 1 plus severity of peripheral artery disease (peak walking time, ankle brachial index and ischemic window).
After adjustment for sex, age, physical activity status and body mass index (Model 1), sedentary behavior remained positively correlated with HsCRP, glucose and fibrinogen; and negatively correlated with HDL-C (P<.05 for all). After adjustment for Model 1 variables plus severity of PAD (Model 2), sedentary behavior remained positively correlated with HsCRP, glucose and fibrinogen; and negatively correlated with HDL-C (P<.05 for all) (Figure 1).
Figure 1. Relationship between biomarkers and sedentary time in patients with symptomatic peripheral artery disease.
Discussion
The main study findings indicated that sedentary behavior was associated with worse inflammation, coagulation, glucose, and lipid metabolism profiles in patients with PAD. The impact of sedentary behavior was independent of sex, age, body mass index, physical activity status and severity of PAD.
Sedentary Behavior Associated with Inflammation and Fibrinogen
This study showed, for the first time, that sedentary behavior was associated with inflammation in patients with symptomatic PAD. Similar results were also observed in older adults, diabetics and obese12-14, 32, which shows the negative impact of sedentary behavior on inflammation in patients with different clinical conditions. In PAD patients, high HsCRP levels have been associated with progression of disease and cardiovascular mortality33. The sedentary time was also associated with high plasma fibrinogen levels. Banerjee et al.,34 observed that high fibrinogen levels was associated with a two-fold increase in the odds of mortality in claudicants. In the present study, each one hour in sedentary time was associated with 0.12 g/L higher fibrinogen levels.
Mechanisms through which sedentary time was associated with inflammation are unclear, however, a recent review study35 claimed that sedentary behaviors lead to an altered myokine response in skeletal muscle, due to fewer skeletal muscle contractions, leading to increased pro-inflammatory status. Another study36 showed that prolonged sitting is associated with the expression of various genes linked to inflammatory responses.
Sedentary Behavior Associated with Cardio-Metabolic Biomarkers
The relationships between sedentary behavior with cardio-metabolic biomarkers, consisting of glucose and HDL-C, were observed in the present study and supports previous work in patients with other clinical conditions. In fact, the National Health and Nutrition Examination Survey (NHANES) study13 observed a positive relation of sedentary behavior with glucose levels and negative relationship with HDL-C levels. Similar results were also observed in the AusDiab study32 and EPIC-Norfolk study37. Review study36 has suggested that prolonged uninterrupted periods of being sedentary results in insufficient skeletal muscle contractions, which suppresses lipoprotein lipase activity, blunts triglyceride uptake, reduces HDL-C levels and glucose load, and increases insulin resistance. In addition, prior bedrest studies38, 39 demonstrated that prolonged sedentary time leads to impaired vascular function manifest as endothelial dysfunction, arterial wall stiffening, and a narrowing of conduit artery diameter. All these factors contribute to the poor health prognosis in patients with PAD. Therefore, the results of this study may explain, at least in part, the strong association between sedentary behavior and cardiovascular mortality observed in older adults and patients with cardiovascular diseases6-8, since inflammatory and cardio-metabolic biomarkers are independent predictors of mortality.
The relationship between time spent in sedentary behavior and worse inflammation, coagulation, glucose, and lipid metabolism profiles observed in this study, reinforces the importance of reducing sedentary time in patients with symptomatic PAD. Previous studies have shown that taking a short break in sitting time has been recommended to reduce the negative effects of sedentary behaviors in different populations13, 40. For example, a previous study40 in overweight adults demonstrated that the inclusion of two minutes of light physical activities every 20 minutes attenuate the inflammatory status of the subjects. Therefore, the inclusion of low intensity physical activity bouts can be potentially useful in patients with functional limitations. However, this suggestion should be further examined in studies with longitudinal design.
Strengths and Limitations
The objective measure of sedentary behavior and the large patient number are aspects that strengthen the study. In addition, this was the first study to analyze the relationship between sedentary behavior and biomarkers in patients with symptomatic PAD. Finally, the relationship of sedentary behavior and biomarkers were adjusted for the physical activity status of the patients, because physical activity is distinct from sedentary behavior, and because physical activity is often related to both sedentary behavior and outcomes by distinct biological mechanisms9. Therefore, the sedentary behavior is related with worse biomarkers, independently of physical activity level in PAD patients.
On the other hand, this study has limitations that should be considered. A non-PAD control group was not included in this study, and therefore it cannot be ascertained whether the associations observed are specific to PAD patients. The cross-sectional design of this study is a limitation, as no causality can be inferred. Patients with severe cardiac disease were excluded in the screening. In addition, this study included only patients with Fontaine Stage II PAD; therefore, the results of this study can only be generalized to our current sample of patients. The use of the step activity monitor to assess sedentary behavior does not quantify the performance of aquatic physical activities or those made with arms, or if the patient is standing. Thus, our definition of sedentary is limited to minutes during the day without any ambulation performed. In addition, cut-off points for sedentary time using the StepWatch have not been established, therefore we chose not to perform analyses using arbitrarily defined sedentary behavior subgroups. Relations were not adjusted for drugs that have a direct impact in the analyzed biomarkers. However, when we tested the influence of risk factors such as hypertension, diabetes, dyslipidemia and heart disease, there was no significant relation, which supports the idea that the drug is not a covariate, given that most patients with the risk factors were on medication.
Conclusion and Clinical Implication
In conclusion, sedentary behavior was associated with worse inflammation, coagulation, glucose, and lipid profiles in patients with symptomatic PAD, independent of sex, age, body mass index, physical activity status and severity of PAD. These results provide evidence of the deleterious consequences of sedentary time on health parameters in these patients. The clinical implication is that interventions need to be developed to reduce the amount of sedentary time in symptomatic patients with PAD, independent of physical activity status. However, in general the relationships found were weak, suggesting that other variables, in addition to sedentary time, are also associated with worse biomarkers in patients with claudication.
Acknowledgments
Funding Sources: Supported by grants from the National Institute on Aging (R01-AG-24296), Oklahoma Center for the Advancement of Science and Technology, and General Clinical Research Center (M01-RR-14467).
Footnotes
Conflict of Interest: The authors declare that they have no conflict of interest
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.McDermott MM, Greenland P, Ferrucci L, Criqui MH, Liu K, Sharma L, et al. Lower extremity performance is associated with daily life physical activity in individuals with and without peripheral arterial disease. J Am Geriatr Soc. 2002;50:247–55. doi: 10.1046/j.1532-5415.2002.50055.x. [DOI] [PubMed] [Google Scholar]
- 2.Spronk S, White JV, Bosch JL, Hunink MG. Impact of claudication and its treatment on quality of life. Semin Vasc Surg. 2007;20:3–9. doi: 10.1053/j.semvascsurg.2007.02.003. [DOI] [PubMed] [Google Scholar]
- 3.Leeper NJ, Myers J, Zhou M, Nead KT, Syed A, Kojima Y, et al. Exercise capacity is the strongest predictor of mortality in patients with peripheral arterial disease. J Vasc Surg. 2013;57:728–33. doi: 10.1016/j.jvs.2012.07.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Depalma RG, Hayes VW, Chow BK, Shamayeva G, May PE, Zacharski LR. Ferritin levels, inflammatory biomarkers, and mortality in peripheral arterial disease: a substudy of the Iron (Fe) and Atherosclerosis Study (FeAST) Trial. J Vasc Surg. 2010;51:1498–503. doi: 10.1016/j.jvs.2009.12.068. [DOI] [PubMed] [Google Scholar]
- 5.Gardner AW, Parker DE, Montgomery PS, Blevins SM, Teague AM, Casanegra AI. Monitored daily ambulatory activity, inflammation, and oxidative stress in patients with claudication. Angiology. 2014;65:491–6. doi: 10.1177/0003319713489769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Grontved A, Hu FB. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA. 2011;305:2448–55. doi: 10.1001/jama.2011.812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, et al. Sedentary Time and Its Association With Risk for Disease Incidence, Mortality, and Hospitalization in Adults: A Systematic Review and Meta-analysis. Ann Intern Med. 2015;162:123–32. doi: 10.7326/M14-1651. [DOI] [PubMed] [Google Scholar]
- 8.Katzmarzyk PT, Church TS, Craig CL, Bouchard C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med Sci Sports Exerc. 2009;41:998–1005. doi: 10.1249/MSS.0b013e3181930355. [DOI] [PubMed] [Google Scholar]
- 9.Page A, Peeters G, Merom D. Adjustment for physical activity in studies of sedentary behaviour. Emerg Themes Epidemiol. 2015;12:10. doi: 10.1186/s12982-015-0032-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sedentary Behaviour Research N. Letter to the editor: standardized use of the terms “sedentary” and “sedentary behaviours”. Appl Physiol Nutr Metab. 2012;37:540–2. doi: 10.1139/h2012-024. [DOI] [PubMed] [Google Scholar]
- 11.Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting: the population health science of sedentary behavior. Exerc Sport Sci Rev. 2010;38:105–13. doi: 10.1097/JES.0b013e3181e373a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gennuso KP, Gangnon RE, Matthews CE, Thraen-Borowski KM, Colbert LH. Sedentary behavior, physical activity, and markers of health in older adults. Med Sci Sports Exerc. 2013;45:1493–500. doi: 10.1249/MSS.0b013e318288a1e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Healy GN, Matthews CE, Dunstan DW, Winkler EA, Owen N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003-06. Eur Heart J. 2011;32:590–7. doi: 10.1093/eurheartj/ehq451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hamer M, Smith L, Stamatakis E. Prospective association of TV viewing with acute phase reactants and coagulation markers: English Longitudinal Study of Ageing. Atherosclerosis. 2015;239:322–7. doi: 10.1016/j.atherosclerosis.2015.02.009. [DOI] [PubMed] [Google Scholar]
- 15.Gardner AW, Montgomery PS, Scott KJ, Afaq A, Blevins SM. Patterns of ambulatory activity in subjects with and without intermittent claudication. J Vasc Surg. 2007;46:1208–14. doi: 10.1016/j.jvs.2007.07.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fontaine R, Kim M, Kieny R. Surgical treatment of peripheral circulation disorders. Helv Chir Acta. 1954;21:499–533. [PubMed] [Google Scholar]
- 17.Gardner AW, Parker DE, Montgomery PS, Blevins SM. Step-monitored home exercise improves ambulation, vascular function, and inflammation in symptomatic patients with peripheral artery disease: a randomized controlled trial. J Am Heart Assoc. 2014;3:e001107. doi: 10.1161/JAHA.114.001107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation. 2011;123:491–8. doi: 10.1161/CIRCULATIONAHA.110.963066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weitz JI, Byrne J, Clagett GP, Farkouh ME, Porter JM, Sackett DL, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:3026–49. doi: 10.1161/01.cir.94.11.3026. [DOI] [PubMed] [Google Scholar]
- 20.Hiatt WR, Marshall JA, Baxter J, Sandoval R, Hildebrandt W, Kahn LR, et al. Diagnostic methods for peripheral arterial disease in the San Luis Valley Diabetes Study. J Clin Epidemiol. 1990;43:597–606. doi: 10.1016/0895-4356(90)90164-k. [DOI] [PubMed] [Google Scholar]
- 21.Gardner AW, Alaupovic P, Parker DE, Montgomery PS, Roof A, Casanegra AI. Apolipoprotein profiles in subjects with and without peripheral artery disease. Vasc Med. 2013;18:129–35. doi: 10.1177/1358863X13489768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Warnick GR, Benderson J, Albers JJ. Dextran sulfate-Mg2+ precipitation procedure for quantitation of high-density-lipoprotein cholesterol. Clin Chem. 1982;28:1379–88. [PubMed] [Google Scholar]
- 23.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 24.Torres JL, Ridker PM. High sensitivity C-reactive protein in clinical practice. Am Heart Hosp J. 2003;1:207–11. doi: 10.1111/j.1541-9215.2003.02109.x. [DOI] [PubMed] [Google Scholar]
- 25.Killewich LA, Gardner AW, Macko RF, Hanna DJ, Goldberg AP, Cox DK, et al. Progressive intermittent claudication is associated with impaired fibrinolysis. J Vasc Surg. 1998;27:645–50. doi: 10.1016/s0741-5214(98)70229-0. [DOI] [PubMed] [Google Scholar]
- 26.Jackson AS, Blair SN, Mahar MT, Wier LT, Ross RM, Stuteville JE. Prediction of functional aerobic capacity without exercise testing. Med Sci Sports Exerc. 1990;22:863–70. doi: 10.1249/00005768-199012000-00021. [DOI] [PubMed] [Google Scholar]
- 27.Gardner AW, Montgomery PS, Parker DE. Physical activity is a predictor of all-cause mortality in patients with intermittent claudication. J Vasc Surg. 2008;47:117–22. doi: 10.1016/j.jvs.2007.09.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Gardner AW, Montgomery PS. Comparison of three blood pressure methods used for determining ankle/brachial index in patients with intermittent claudication. Angiology. 1998;49:723–8. doi: 10.1177/000331979804901003. [DOI] [PubMed] [Google Scholar]
- 29.Feinberg RL, Gregory RT, Wheeler JR, Snyder SO, Jr, Gayle RG, Parent FN, 3rd, et al. The ischemic window: a method for the objective quantitation of the training effect in exercise therapy for intermittent claudication. J Vasc Surg. 1992;16:244–50. doi: 10.1067/mva.1992.36947. [DOI] [PubMed] [Google Scholar]
- 30.Gardner AW, Skinner JS, Cantwell BW, Smith LK. Progressive vs single-stage treadmill tests for evaluation of claudication. Med Sci Sports Exerc. 1991;23:402–8. [PubMed] [Google Scholar]
- 31.Gardner AW. Reliability of transcutaneous oximeter electrode heating power during exercise in patients with intermittent claudication. Angiology. 1997;48:229–35. doi: 10.1177/000331979704800305. [DOI] [PubMed] [Google Scholar]
- 32.Howard BJ, Balkau B, Thorp AA, Magliano DJ, Shaw JE, Owen N, et al. Associations of overall sitting time and TV viewing time with fibrinogen and C reactive protein: the AusDiab study. Br J Sports Med. 2015;49:255–8. doi: 10.1136/bjsports-2013-093014. [DOI] [PubMed] [Google Scholar]
- 33.McDermott MM, Lloyd-Jones DM. The role of biomarkers and genetics in peripheral arterial disease. J Am Coll Cardiol. 2009;54:1228–37. doi: 10.1016/j.jacc.2009.04.081. [DOI] [PubMed] [Google Scholar]
- 34.Banerjee AK, Pearson J, Gilliland EL, Goss D, Lewis JD, Stirling Y, et al. A six year prospective study of fibrinogen and other risk factors associated with mortality in stable claudicants. Thromb Haemost. 1992;68:261–3. [PubMed] [Google Scholar]
- 35.Pedersen BK, Febbraio MA. Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nat Rev Endocrinol. 2012;8:457–65. doi: 10.1038/nrendo.2012.49. [DOI] [PubMed] [Google Scholar]
- 36.Latouche C, Jowett JB, Carey AL, Bertovic DA, Owen N, Dunstan DW, et al. Effects of breaking up prolonged sitting on skeletal muscle gene expression. J Appl Physiol (1985) 2013;114:453–60. doi: 10.1152/japplphysiol.00978.2012. [DOI] [PubMed] [Google Scholar]
- 37.Jakes RW, Day NE, Khaw KT, Luben R, Oakes S, Welch A, et al. Television viewing and low participation in vigorous recreation are independently associated with obesity and markers of cardiovascular disease risk: EPIC-Norfolk population-based study. Eur J Clin Nutr. 2003;57:1089–96. doi: 10.1038/sj.ejcn.1601648. [DOI] [PubMed] [Google Scholar]
- 38.Nosova EV, Yen P, Chong KC, Alley HF, Stock EO, Quinn A, et al. Short-term physical inactivity impairs vascular function. J Surg Res. 2014;190:672–82. doi: 10.1016/j.jss.2014.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Palombo C, Morizzo C, Baluci M, Lucini D, Ricci S, Biolo G, et al. Large artery remodeling and dynamics following simulated microgravity by prolonged head-down tilt bed rest in humans. Biomed Res Int. 2015;2015:342565. doi: 10.1155/2015/342565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Howard BJ, Fraser SF, Sethi P, Cerin E, Hamilton MT, Owen N, et al. Impact on hemostatic parameters of interrupting sitting with intermittent activity. Med Sci Sports Exerc. 2013;45:1285–91. doi: 10.1249/MSS.0b013e318285f57e. [DOI] [PubMed] [Google Scholar]