

Abstract
Background
Elevated serum calcium concentrations are associated with vascular calcification and cardiovascular disease. It is unknown whether there is a relationship between high-normal serum calcium levels and sub-clinical vascular effects. We investigated the association between serum calcium and carotid plaque thickness, a powerful early predictor of clinical coronary and cerebrovascular events.
Methods
Epidemiological study of 1194 subjects from the Northern Manhattan Study cohort, a prospective community-based study designed to investigate risk factors for vascular disease in different race-ethnic groups.
Results
Subjects with carotid plaque had higher corrected serum calcium levels within the normal range than those without carotid plaque (2.21 ± .09 vs. 2.19 ± .09 mmol/L, p<0.002). The relationship between carotid plaque and serum calcium persisted after adjustment for traditional cardiovascular risk factors. Subjects in the top quintile of maximal carotid plaque thickness (≥ 1.7 mm) were more likely to be in the highest quintile of serum calcium level (OR=1.64, 95% CI=1.17 to 2.29, p< 0.004). The interaction of age and corrected serum calcium was the most significant predictor of carotid plaque thickness when traditional vascular risk factors were considered (p<0.001).
Conclusions
Serum calcium levels in a multi-ethnic population of older men and women were positively associated with carotid plaque thickness, a powerful early predictor of clinical coronary and cerebrovascular events.
Introduction
Elevated serum calcium levels have been suggested to be a risk factor for accelerated coronary atherosclerosis [1]. In the setting of overt hypercalcemia, increased deposition of calcium occurs in the fibrous skeleton of the heart and valvular cusps, as well as in the coronary arteries and myocardial fibers [2]. However, even when serum calcium is within the normal range, high-normal serum calcium values appear to be associated with increased cardiovascular morbidity. Large-scale epidemiologic data from Sweden have shown that in middle-aged men, serum calcium levels are an independent, prospective risk factor for myocardial infarction [3, 4] and high-normal serum calcium levels are associated with increased cardiovascular mortality [5]. Recent data from the Women's Health Initiative, which raise questions about the risks and benefits of calcium supplementation, increase the importance of investigating the association between serum calcium levels and pre-clinical cardiovascular disease. [6].
Previous studies addressing serum calcium and cardiovascular risk assessed mortality or cardiovascular outcomes in Scandinavian cohorts. Sub-clinical markers of cardiovascular disease, however, are known to be highly predictive of such outcomes. A recent study found carotid artery plaque burden to be an important independent risk factor for subsequent cardiovascular mortality [7]. Carotid artery plaque and carotid intima-media thickness (IMT), as detected by non-invasive high-resolution ultrasound, are well known markers of systemic sub-clinical atherosclerosis. In large population studies, these measures have been shown to be strong predictors of future fatal and non-fatal myocardial infarct (MI) and stroke [8, 9]. Of the two, several studies suggest that carotid artery plaque thickness may be a more powerful predictor of vascular outcomes than IMT [10, 11]. There are no data on the association of a marker of sub-clinical vascular disease such as carotid plaque thickness with serum calcium levels. We therefore evaluated whether higher serum calcium levels, within the normal range, would be associated with increased carotid artery plaque thickness in a community dwelling stroke-free American population.
Methods
Study Subjects
The study population was obtained from the Northern Manhattan Study (NOMAS), a prospective community-based study designed to investigate vascular risk factors and the incidence of vascular events in different race-ethnic groups in northern Manhattan [12]. NOMAS follows 3298 stroke-free adults. For the current study, only subjects who underwent carotid duplex Doppler sonography examination, serum calcium and albumin measurement at study entry were included. Clinical information included age, sex, race and presence of cardiovascular risk factors (hypertension [history of hypertension or systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg], diabetes mellitus [fasting blood glucose level ≥ 6.99 mmol/L or the subject's self-report of diabetes, insulin use, or oral hypoglycemic use], pre-existing heart disease [subject told of or currently taking medication for the diagnosis], cholesterol level, tobacco use within the past 5 years and alcohol consumption [light:<1drink monthly, moderate:< 2 drinks daily or heavy:> 2 drinks daily]). The study was approved by the Columbia Institutional Review Board and patients gave written informed consent.
Carotid Ultrasound: Maximum Carotid Artery Plaque Thickness (MCPT)
Carotid artery plaque was assessed by high-resolution B-mode ultrasound according to a standard scanning and reading protocol as previously described [13, 14] on a GE LogIQ 700 system with a multifrequency 9/13-MHz linear-array transducer. With the subject in a supine position, the extracranial carotid arteries were imaged in short axial and long longitudinal planes (anterior, lateral and posterior views). Internal and common carotid arteries as well as the bifurcations were examined for the presence of atherosclerotic plaque, defined as an area of wall thickening or protrusion in the lumen more than 50% greater than surrounding wall thickness. MCPT (mm) was measured at the highest plaque prominence in any of the three carotid artery segments assessed from the digitized multi-angled images (Figure 1). If no plaque was identified, plaque thickness was recorded as zero. If plaque was present in any segments, the plaque boundaries were traced and MCPT was calculated using the semi-automatic IMAGE-Pro V.5.2 software. MCPT and carotid segment location for each plaque was recorded.
Figure 1. Measurement of Maximal Carotid Plaque Thickness (MCPT).

ICA indicates internal carotid artery; ECA, external carotid artery; and CCA, common carotid artery. MCPT (maximal carotid plaque thickness) is defined as maximum distance between 2 traced plaque boundaries in a defined carotid segment. MCPT is measured by a semi-automatic specialized vascular image system.
Serum Calcium and Albumin
Measurements of serum calcium and albumin were performed by standard autoanalyzer techniques (Technicon Instruments, Tarrytown, NY). The serum calcium concentration was corrected for serum albumin by the formula: corrected [Ca] = measured total [Ca] + 0.8 × (4.0- [alb]). The criteria for inclusion (normal concentration of serum calcium [2.05 – 2.60 mmol/L (8.2-10.4 mg/dl)]) were based on serum calcium adjusted for albumin.
Statistical Analysis
All continuous data are presented as mean value ± SD, and all categorical data are reported as percentage or absolute number. Student's t tests and Chi-square tests were used to assess differences between groups. A multivariate analysis of variance was performed to test whether any of the characteristics of the study population differed between subjects with and without detectable carotid plaque. An overall finding of statistical significance (p < 0.05) was interpreted to justify analysis of between group differences for each characteristic. The presence or absence of carotid artery plaque, MCPT as a continuous measure, and MCPT as a categorical measure (top quintile of MCPT [≥ 1.7 mm]) were analyzed separately. The multivariate relationship among variables was evaluated by multiple regression when MCPT was considered a continuous outcome and logistic regression analyses when MCPT was treated as a categorical outcome (1.7 mm or greater compared to zero). Multivariate analyses were adjusted for age, sex, race and vascular risk factors including hypertension, diabetes mellitus, pre-existing heart disease, LDL, HDL, tobacco use and alcohol consumption. The role of sex in the interaction of corrected calcium and plaque was assessed by a mixed model analysis with fixed effects for presence or absence of plaque, sex and plaque by sex interaction. A P value of less than 0.05 was considered significant. All statistical analyses were performed using SAS (version 9.0).
Role of the Funding Source
The National Institutes of Health/National Institute of Diabetes and Digestive Diseases and National Institutes of Health/National Institute of Neurological Disorders and Stroke provided funding for the study. The funding sources had no role in the design, conduct or reporting of the study.
Results
Baseline Characteristics of the Study Population
Of the 3298 subjects in NOMAS, 2000 chosen at random had carotid duplex Doppler sonography. Of those, 1350 had measurement of serum calcium; of those, 1277 also had measurement of serum albumin. The subjects who had measurement of serum calcium and albumin were representative of the overall cohort that underwent Doppler sonography with respect to demographics, vascular risk factors and distribution of plaque. Subjects (N=83; 6.5%) were excluded when serum calcium was outside the normal range (2.05 – 2.60 mmol/L [8.2-10.4 mg/dl]; 80 subjects with low serum calcium and 3 subjects with elevated calcium). Baseline clinical characteristics and laboratory data for the resulting study population (n=1194) are shown in Table 1. Carotid plaque was detected on ultrasound in 57% of the subjects (n= 678). A MANOVA F-test showed that the vector of baseline cardiovascular risk measures differed significantly between groups defined by the presence or absence of detectable carotid plaque (p < 0.001). The results of T-tests are shown to identify the measures responsible for the significant multivariate comparison. Those with plaque were older (70 ± 9 vs. 64 ± 8 yrs, p <0.001), more likely to have pre-existing heart disease, and more frequently hypertensive, diabetic or smokers.
Table 1. Characteristics of the Study Population.
| Variable | All Subjects (n= 1194) | Subjects with plaque (n= 678) | Subjects without plaque (n= 516) | P-value | |
|---|---|---|---|---|---|
| Age (yr) | 68 ± 9 | 70 ± 9 | 64 ± 8 | <0.001 | |
| Male (%) | 39 | 40 | 38 | NS | |
| Race (%) | Hispanic | 53 | 46 | 62 | |
| Black | 22 | 25 | 19 | <0.001 | |
| White | 22 | 27 | 15 | ||
| Other | <3 | 2 | 4 | ||
| Hypertension (%) | 72 | 76 | 66 | <0.001 | |
| Diabetes mellitus (%) | 23 | 26 | 19 | <0.008 | |
| Current smoker (%) | 14 | 16 | 11 | <0.04 | |
| Pre-existing heart disease (%) | 20 | 24 | 15 | <0.001 | |
| Alcohol use (≥ 2 drinks/d; %) | 42 | 41 | 43 | NS | |
| LDL (mmol/L)* | 3.37± .96 | 3.39± .98 | 3.34 ± .93 | NS | |
| HDL (mmol/L)* | 1.19 ± .36 | 1.22± .36 | 1.19 ± .36 | NS | |
| Serum Calcium (mmol/L) | 2.20 ± .09 (8.81 ± 0.36 mg/dl) | 2.21 ± .09 (8.84 ± 0.37 mg/dl) | 2.19 ± .09 (8.77 ± 0.36 mg/dl) | <0.002 | |
| MCPT (mm) | 0.97 ± 1.05 | 1.70 ± 0.82 | 0 | ||
± SD for all values
for traditional units divide by .0259
Calcium and Maximum Carotid Plaque Thickness
Mean corrected serum calcium was 2.20 ± .09 mmol/L (8.81 ± 0.36 mg/dl) and mean MCPT was 0.97 ± 1.05 mm. Serum calcium was higher among subjects with plaque than without (2.21 ± .09 vs. 2.19 ± .09 mmol/L [8.84 ± 0.37 vs. 8.77 ± 0.36 mg/dl]; p<0.002). The association between calcium and MCPT is shown in Figure 2. Although there were individuals without plaque throughout most of the range of serum calcium (Figure 2, shaded area), those without plaque tended to cluster in the lower half of the normal range of serum calcium. Within the entire cohort (with plaque and without), when corrected serum calcium was divided into quintiles (ranges: 2.05-2.12, 2.13-2.17, 2.18-2.22, 2.23-2.27, 2.28-2.60 mmol/L; [8.20-8.49, 8.50-8.69, 8.70-8.89, 8.90-9.09, 9.10-10.39 mg/dl]), a mean MCPT difference of 0.33 mm was found for the highest quintile of calcium as compared to the lowest (1.17 ± 1.17 mm vs. 0.84 ± 1.03 mm; p < 0.002; Figure 3). When MCPT was treated as a categorical variable within the entire cohort, those in the top quintile of MCPT (≥ 1.7 mm) were more likely to be in the highest quintile of serum calcium level (OR=1.64, 95% CI=1.17 to 2.29, p< 0.004; Figure 4). When only those with plaque were considered, the average MCPT increased with each corrected calcium quintile, in a step-wise manner. The one exception was that the average MCPT of subjects in the lowest quintile of corrected serum calcium was insignificantly greater than that found in the next quintile.
Figure 2. Distribution of Corrected Serum Calcium and MCPT Among All Subjects (n=1194).
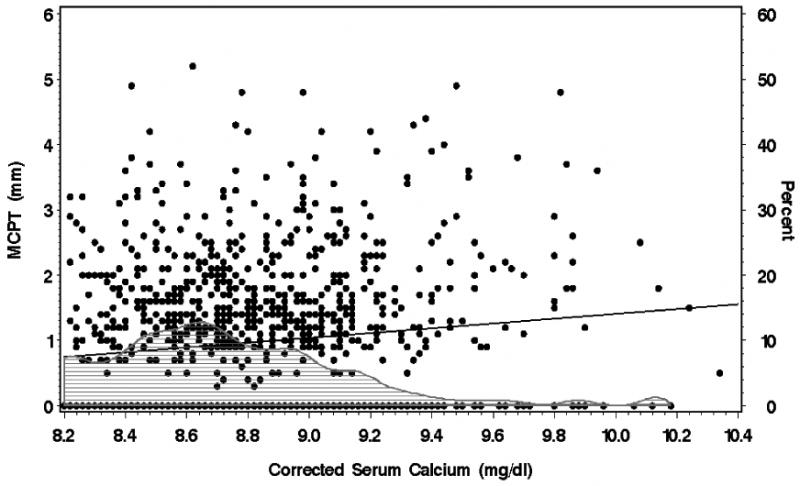
The regression line reflects the overall relationship between corrected calcium and MCPT (maximal carotid plaque thickness), in subjects both with and without plaque (r = +0.12, p <0.001). The shaded area specifies the percent of subjects without plaque (using the right axis) at each level of corrected calcium. To convert corrected serum calcium to mmol/L, multiply by 0.25.
Figure 3. Carotid Plaque Thickness by Calcium Quintile.

The average MCPT (maximal carotid plaque thickness) (± SD) value in the highest corrected calcium quintile is significantly higher (p=0.002) than the MCPT in the lowest corrected calcium quintile.
Figure 4. Top Quintile Plaque Thickness Likely in Highest Quintile Serum Calcium.

Subjects in the top quintile of MCPT (maximal carotid plaque thickness) (≥ 1.7 mm) were 64% more likely to be in the highest quintile of serum calcium level (2.28- 2.60 mmol/L [9.10 – 10.39 mg/dl]).
The association between corrected calcium and plaque did not vary by sex. MCPT was not significantly different between men and women (1.022 ± 1.11 vs. 0.931 ± 1.03 mm, respectively; p=0.15) and mean corrected calcium in both sexes was lower in those without plaque than with plaque (men: 2.17 ± 0.09 vs. 2.19 ± 0.08 mmol/L, p<0.04; women: 2.20 ± 0.09 vs. 2.22 ± 0.09 mmol/L, p<0.009). A mixed model analysis with fixed effects for presence of MCPT, sex and plaque by sex interaction did not show a significant difference in plaque by sex interaction (p=0.91).
Stepwise multiple regression models were performed to assess the interaction of factors in predicting MCPT. Serum calcium, age, race, sex and cardiovascular risk factors and their second order interactions were entered in the model. The mathematical model showed that the interaction of age and corrected serum calcium was the most significant predictor of MCPT, accounting for 7% of the variance in MCPT (p<0.001). Those with the highest age and highest corrected serum calcium were most likely to have the highest MCPT. Furthermore, this relationship persisted across all age groups regardless of level of cardiovascular risk (presence or absence of smoking, diabetes, hypertension, pre-existing heart disease, and highest LDL and lowest HDL of the study subjects).
Relationship Between Serum Calcium and Other Variables
Risk Factors for Atherosclerosis
Serum calcium was not associated with the presence of hypertension, pre-existing cardiac disease, current smoking, or LDL level. Diabetics had higher serum calcium than non-diabetics (2.22 ± .10 vs. 2.20 ± .09 mmol/L; p<0.003) and moderate alcohol consumption was associated with lower serum calcium than light alcohol consumption (2.21 ± .10 vs. 2.19 ± .08 mmol/L, respectively, p < 0.001).
Race
Corrected serum calcium levels differed by race. African-American subjects had mean values (2.23 mmol/L) that were 0.03 mmol/L (0.01– 0.05 95% CI) higher than those in Caucasians and 0.04 mmol/L (0.01 – 0.06 95% CI) higher than calcium levels in Hispanics (P < 0.001). Serum calcium and MCPT were weakly but significantly associated in African-Americans and Caucasian individuals (r = +0.17, p < 0.005), but not in Hispanics (r = +0.04, p = 0.37). Regression analysis controlling for age and sex showed that the relationship between corrected serum calcium and MCPT differed across the races. The increase in MCPT per mg/dl increase in calcium was lowest in Hispanics (0.106 ± .11 mm), highest in African-Americans (0.304 ± .15mm) and intermediate in Caucasians (0.252 ± .18 mm).
Discussion
We found that serum calcium levels in multiethnic, community dwelling, normocalcemic individuals are positively associated with carotid plaque thickness, a powerful early predictor of systemic atherosclerosis and clinical coronary and cerebrovascular events. Individuals with higher corrected serum calcium concentration within the normal range were more likely to have carotid plaque that those with lower calcium levels. The most significant predictor of MCPT was the interaction of age and corrected serum calcium.
The association between serum calcium and cardiovascular or cerebrovascular disease risk has been described in large Swedish epidemiologic studies in middle-aged Caucasian men [3-5]. An association between serum calcium and carotid plaque has also been described in populations with abnormal calcium metabolism. In primary hyperparathyroidism, markedly hypercalcemic patients had increased IMT as compared to normocalcemic controls [15]. Data in those with milder calcium elevations did not confirm these findings [16], but these data were limited, since IMT was measured in the common carotid artery, rather than the internal carotid artery, a more common site for atherosclerotic plaque [11]. Hemodialysis patients, another population with abnormal calcium metabolism [17], have also been found to have a positive association between serum calcium and carotid plaque [18]. Our finding extends this association to healthy normocalcemic men and women.
It could be argued that our patients might not be truly normocalcemic if their ionized calcium levels were elevated. Although ionized calcium data are unavailable in this cohort, we controlled for this factor to the extent possible by using corrected, rather than total, serum calcium levels. We also considered the possibility that serum calcium is linked with some of the conventional risk factors for cardiovascular disease, such as diabetes mellitus, glucose levels, hypertension, total cholesterol, triglycerides, and lipids and thus might not be a true independent risk factor. We therefore considered the possibility that higher calcium levels might be a surrogate for state(s) that promote atherogenesis. Although we found that serum calcium was associated with diabetes mellitus, even after adjusting for diabetes and other risk factors, serum calcium remained an independent risk factor for increased plaque.
Racial breakdown showed that the association between serum calcium and plaque persisted among the different ethnic groups. Although one might expect that African-American individuals might not exhibit the association, due to potentially greater vitamin D resistance and lower serum calcium levels [19], contrary to expectations, they in fact had the highest serum calcium levels and the highest rate of increase in MCPT per mg/dl increase in corrected calcium. Whether a factor other than vitamin D is associated in African-Americans with serum calcium and plaque increase is unknown.
Any explanation for a potential relationship between serum calcium and plaque remains speculative. Calcified atherosclerotic arteries contain tissue that is histologically similar to bone [20, 21]. It is conceivable that a higher serum calcium might predispose these cells (known as vascular calcifying cells) to become more like osteoblasts [22] and that mineral deposition in the vessel wall is more likely to occur if local ionic concentrations exceed the salt solubility product. A higher ambient calcium concentration might alter the vascular microenvironment to become more like bone and favor plaque formation. In addition, a mediating factor might be present linking increasing serum calcium levels with vascular calcification. Calciotropic hormones were not measured, but vasodilatory [23] and inotropic [2] properties of PTH might theoretically afford vascular protection to individuals with low-normal serum calcium values whose PTH levels are high-normal. 1,25-dihyroxyvitamin D (1,25(OH)2D) [24, 25] and osteoprotegerin [26] might also play roles in vascular calcification. The association between serum calcium and plaque implies that the plaque is calcified, but there are no available data to support this. Even if calcified plaque were to be demonstrated, there is ongoing debate whether calcification is a marker for an unstable plaque [27] or whether it might in fact stabilize the plaque [28, 29].
Bisphosphonates have been reported to have potential salutary effects on measures of vascular disease, such as coronary calcification scores or carotid IMT, in patients on long-term hemodialysis [30] or with type 2 diabetes mellitus [31], respectively. Although the mechanisms by which bisphosphonates may inhibit atherosclerosis remain to be elucidated, it is possible that they might trigger beneficial effects on the calcium deposits in the arterial wall [32].
There are several limitations to this study. In this free-living older population, serum calcium levels were not equally distributed throughout the normal range, with the largest group being clustered at the lower end of normal. This might be attributable to differences from the population in which the laboratory normal range was derived, which included younger individuals and was less multi-ethnic. Furthermore, as mentioned above, there are no data on calciotropic hormones in these subjects, or on the inflammatory cytokines known to affect both the skeleton and vascular calcification. In addition, phosphorus levels are not available, and assessment of the relationship between the calcium-phosphate product and carotid plaque would be of interest, as it is in patients with renal failure. Moreover, because this is a cross-sectional study, cause and effect cannot be discerned. Whether these subjects have had a change in serum calcium over the years is unknown. In atherosclerotic plaque calcification, it might not be the static measurement of the serum calcium that is important, but rather the change in serum calcium over time. In any case, the notion that calcification of vascular plaque can be explained as a purely stoichiometric phenomenon is clearly simplistic. In addition, it is likely that these findings are more important on a population rather than on an individual level. The difference in serum calcium between those with and without plaque (2.21 vs.2.19 mmol/L [8.84 vs. 8.87 mg/dl]) was small and would not be clinically relevant in an individual. However it is noteworthy that the difference in serum calcium of precisely the same magnitude was reported in a prospective study of 2183 men followed for 18 years for the development of myocardial infarction (developed MI: calcium 2.37 +/- 0.09 SD vs no MI: 2.35 +/- 0.09 mmol/l; p < 0.03) [3].
This study is not designed to elucidate potential underlying pathophysiologic abnormalities that could account for the observations. That there is a mediating step between calcium and plaque is highlighted by the finding that 43% of the subjects had no plaque, yet had a similar range of serum calcium levels. Since the subjects without plaque were younger, it is possible that they were in a pre-clinical stage with early cardiovascular abnormalities pre-disposing them to plaque that has not yet calcified. It is also possible that the relationship between calcium and plaque is non-linear, as was the case in a study of patients with primary hyperparathyroidism, in which cardiovascular mortality was similar among those in the 3 lower quartiles of serum calcium, but was increased among patients in the highest quartile [33]. There could well be a threshold effect of serum calcium, below which cardiovascular effects might not occur.
It is important to note that we did not account for calcium intake in this population. However, normal dietary calcium intake does not elevate blood calcium levels. Indeed, a recent assessment of the effect of calcium intake on mineral metabolism found no difference in ionized calcium levels in those with low, modest or high calcium intake [34]. Although the Women's Health Initiative recently found an increased risk of kidney stones in postmenopausal women on calcium and vitamin D supplements [6], there is no evidence that postmenopausal women who take such supplements have significant increases in their serum calcium concentration. The data from our study, therefore, do not in themselves justify a revision of current views of dietary or supplemental calcium intake. Nevertheless, the questions raised by the WHI data in conjunction with these observations highlight the need for further investigation of serum calcium and pre-clinical atherosclerosis.
In conclusion, serum calcium levels in a multi-ethnic population of older men and women are positively associated with carotid plaque thickness, a powerful early predictor of clinical coronary and cerebrovascular events. Subjects with no carotid plaque had lower corrected serum calcium levels within the normal range than did those who had carotid plaque, an association that persisted after adjustment for other cardiovascular risk factors. Although accounting for only a small proportion of the variance, the interaction of age and corrected serum calcium was the most significant predictor of carotid plaque thickness when traditional vascular risk factors were considered. Although these data do not presuppose a causal relationship between serum calcium and carotid plaque thickness, it is clear that further studies are needed to investigate the mechanism of this association, and its clinical consequences.
Acknowledgments
Grant Support: National Institutes of Health/National Institute of Diabetes and Digestive Diseases DK66329 and DK32333; and National Institutes of Health/National Institute of Neurological Disorders and Stroke grant NS-R01-29993.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Roberts WC, Waller BF. Effect of chronic hypercalcemia on the heart. An analysis of 18 necropsy patients. Am J Med. 1981;71(3):371–84. doi: 10.1016/0002-9343(81)90163-7. [DOI] [PubMed] [Google Scholar]
- 2.Stefenelli T, Abela C, Frank H, Koller-Strametz J, Globits S, Bergler-Klein J, Niederle B. Cardiac abnormalities in patients with primary hyperparathyroidism: implications for follow-up. J Clin Endocrinol Metab. 1997;82(1):106–12. doi: 10.1210/jcem.82.1.3666. [DOI] [PubMed] [Google Scholar]
- 3.Lind L, Skarfors E, Berglund L, Lithell H, Ljunghall S. Serum calcium: a new, independent, prospective risk factor for myocardial infarction in middle-aged men followed for 18 years. J Clin Epidemiol. 1997;50(8):967–73. doi: 10.1016/s0895-4356(97)00104-2. [DOI] [PubMed] [Google Scholar]
- 4.Jorde R, Sundsfjord J, Fitzgerald P, Bonaa KH. Serum calcium and cardiovascular risk factors and diseases: the Tromso study. Hypertension. 1999;34(3):484–90. doi: 10.1161/01.hyp.34.3.484. [DOI] [PubMed] [Google Scholar]
- 5.Leifsson BG, Ahren B. Serum calcium and survival in a large health screening program. J Clin Endocrinol Metab. 1996;81(6):2149–53. doi: 10.1210/jcem.81.6.8964843. [DOI] [PubMed] [Google Scholar]
- 6.Jackson RD, LaCroix AZ, Gass M, Wallace RB, Robbins J, Lewis CE, Bassford T, Beresford SA, Black HR, Blanchette P, Bonds DE, Brunner RL, Brzyski RG, Caan B, Cauley JA, Chlebowski RT, Cummings SR, Granek I, Hays J, Heiss G, Hendrix SL, Howard BV, Hsia J, Hubbell FA, Johnson KC, Judd H, Kotchen JM, Kuller LH, Langer RD, Lasser NL, Limacher MC, Ludlam S, Manson JE, Margolis KL, McGowan J, Ockene JK, O'Sullivan MJ, Phillips L, Prentice RL, Sarto GE, Stefanick ML, Van Horn L, Wactawski-Wende J, Whitlock E, Anderson GL, Assaf AR, Barad D. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006;354(7):669–83. doi: 10.1056/NEJMoa055218. [DOI] [PubMed] [Google Scholar]
- 7.Stork S, van den Beld AW, von Schacky C, Angermann CE, Lamberts SW, Grobbee DE, Bots ML. Carotid artery plaque burden, stiffness, and mortality risk in elderly men: a prospective, population-based cohort study. Circulation. 2004;110(3):344–8. doi: 10.1161/01.CIR.0000134966.10793.C9. [DOI] [PubMed] [Google Scholar]
- 8.Chambless LE, Folsom AR, Clegg LX, Sharrett AR, Shahar E, Nieto FJ, Rosamond WD, Evans G. Carotid wall thickness is predictive of incident clinical stroke: the Atherosclerosis Risk in Communities (ARIC) study. Am J Epidemiol. 2000;151(5):478–87. doi: 10.1093/oxfordjournals.aje.a010233. [DOI] [PubMed] [Google Scholar]
- 9.O'Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK., Jr Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med. 1999;340(1):14–22. doi: 10.1056/NEJM199901073400103. [DOI] [PubMed] [Google Scholar]
- 10.Ebrahim S, Papacosta O, Whincup P, Wannamethee G, Walker M, Nicolaides AN, Dhanjil S, Griffin M, Belcaro G, Rumley A, Lowe GD. Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women: the British Regional Heart Study. Stroke. 1999;30(4):841–50. doi: 10.1161/01.str.30.4.841. [DOI] [PubMed] [Google Scholar]
- 11.Spence JD, Eliasziw M, DiCicco M, Hackam DG, Galil R, Lohmann T. Carotid plaque area: a tool for targeting and evaluating vascular preventive therapy. Stroke. 2002;33(12):2916–22. doi: 10.1161/01.str.0000042207.16156.b9. [DOI] [PubMed] [Google Scholar]
- 12.Sacco RL, Roberts JK, Boden-Albala B, Gu Q, Lin IF, Kargman DE, Berglund L, Hauser WA, Shea S, Paik MC. Race-ethnicity and determinants of carotid atherosclerosis in a multiethnic population. The Northern Manhattan Stroke Study. Stroke. 1997;28(5):929–35. doi: 10.1161/01.str.28.5.929. [DOI] [PubMed] [Google Scholar]
- 13.Desvarieux M, Demmer RT, Rundek T, Boden-Albala B, Jacobs DR, Jr, Papapanou PN, Sacco RL. Relationship between periodontal disease, tooth loss, and carotid artery plaque: the Oral Infections and Vascular Disease Epidemiology Study (INVEST) Stroke. 2003;34(9):2120–5. doi: 10.1161/01.STR.0000085086.50957.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Elkind MS, Cheng J, Boden-Albala B, Rundek T, Thomas J, Chen H, Rabbani LE, Sacco RL. Tumor necrosis factor receptor levels are associated with carotid atherosclerosis. Stroke. 2002;33(1):31–7. doi: 10.1161/hs0102.100531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nuzzo V, Tauchmanova L, Fonderico F, Trotta R, Fittipaldi MR, Fontana D, Rossi R, Lombardi G, Trimarco B, Lupoli G. Increased intima-media thickness of the carotid artery wall, normal blood pressure profile and normal left ventricular mass in subjects with primary hyperparathyroidism. Eur J Endocrinol. 2002;147(4):453–9. doi: 10.1530/eje.0.1470453. [DOI] [PubMed] [Google Scholar]
- 16.Fallo F, Camporese G, Capitelli E, Andreozzi GM, Mantero F, Lumachi F. Ultrasound evaluation of carotid artery in primary hyperparathyroidism. J Clin Endocrinol Metab. 2003;88(5):2096–9. doi: 10.1210/jc.2002-021837. [DOI] [PubMed] [Google Scholar]
- 17.Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, Wang Y, Chung J, Emerick A, Greaser L, Elashoff RM, Salusky IB. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342(20):1478–83. doi: 10.1056/NEJM200005183422003. [DOI] [PubMed] [Google Scholar]
- 18.Malatino LS, Benedetto FA, Mallamaci F, Tripepi G, Zoccali C, Parlongo S, Cutrupi S, Marino C, Panuccio V, Garozzo M, Candela V, Bellanuova I, Cataliotti A, Rapisarda F, Fatuzzo P, Bonanno G, Seminara G, Stancanelli B, Tassone F, Labate C. Smoking, blood pressure and serum albumin are major determinants of carotid atherosclerosis in dialysis patients. CREED Investigators. Cardiovascular Risk Extended Evaluation in Dialysis patients. J Nephrol. 1999;12(4):256–60. [PubMed] [Google Scholar]
- 19.Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. Lancet. 1982;1(8263):74–6. doi: 10.1016/s0140-6736(82)90214-8. [DOI] [PubMed] [Google Scholar]
- 20.Abedin M, Tintut Y, Demer LL. Vascular calcification: mechanisms and clinical ramifications. Arterioscler Thromb Vasc Biol. 2004;24(7):1161–70. doi: 10.1161/01.ATV.0000133194.94939.42. [DOI] [PubMed] [Google Scholar]
- 21.Demer LL, Tintut Y. Mineral exploration: search for the mechanism of vascular calcification and beyond: the 2003 Jeffrey M. Hoeg Award lecture. Arterioscler Thromb Vasc Biol. 2003;23(10):1739–43. doi: 10.1161/01.ATV.0000093547.63630.0F. [DOI] [PubMed] [Google Scholar]
- 22.Schinke T, McKee MD, Karsenty G. Extracellular matrix calcification: where is the action? Nat Genet. 1999;21(2):150–1. doi: 10.1038/5928. [DOI] [PubMed] [Google Scholar]
- 23.Ogino K, Burkhoff D, Bilezikian JP. The hemodynamic basis for the cardiac effects of parathyroid hormone (PTH) and PTH-related protein. Endocrinology. 1995;136(7):3024–30. doi: 10.1210/endo.136.7.7789328. [DOI] [PubMed] [Google Scholar]
- 24.Bajwa GS, Morrison LM, Ershoff BH. Induction of aortic and coronary athero-arteriosclerosis in rats fed a hypervitaminosis D, cholesterol-containing diet. Proc Soc Exp Biol Med. 1971;138(3):975–82. doi: 10.3181/00379727-138-36030. [DOI] [PubMed] [Google Scholar]
- 25.Niederhoffer N, Bobryshev YV, Lartaud-Idjouadiene I, Giummelly P, Atkinson J. Aortic calcification produced by vitamin D3 plus nicotine. J Vasc Res. 1997;34(5):386–98. doi: 10.1159/000159247. [DOI] [PubMed] [Google Scholar]
- 26.Browner WS, Lui LY, Cummings SR. Associations of serum osteoprotegerin levels with diabetes, stroke, bone density, fractures, and mortality in elderly women. J Clin Endocrinol Metab. 2001;86(2):631–7. doi: 10.1210/jcem.86.2.7192. [DOI] [PubMed] [Google Scholar]
- 27.Farb A, Burke AP, Tang AL, Liang TY, Mannan P, Smialek J, Virmani R. Coronary plaque erosion without rupture into a lipid core. A frequent cause of coronary thrombosis in sudden coronary death. Circulation. 1996;93(7):1354–63. doi: 10.1161/01.cir.93.7.1354. [DOI] [PubMed] [Google Scholar]
- 28.Doherty TM, Wong ND, Shavelle RM, Tang W, Detrano RC. Coronary heart disease deaths and infarctions in people with little or no coronary calcium. Lancet. 1999;353(9146):41–2. doi: 10.1016/S0140-6736(05)74866-2. [DOI] [PubMed] [Google Scholar]
- 29.Cheng GC, Loree HM, Kamm RD, Fishbein MC, Lee RT. Distribution of circumferential stress in ruptured and stable atherosclerotic lesions. A structural analysis with histopathological correlation. Circulation. 1993;87(4):1179–87. doi: 10.1161/01.cir.87.4.1179. [DOI] [PubMed] [Google Scholar]
- 30.Nitta K, Akiba T, Suzuki K, Uchida K, Watanabe R, Majima K, Aoki T, Nihei H. Effects of cyclic intermittent etidronate therapy on coronary artery calcification in patients receiving long-term hemodialysis. Am J Kidney Dis. 2004;44(4):680–8. [PubMed] [Google Scholar]
- 31.Koshiyama H, Nakamura Y, Tanaka S, Minamikawa J. Decrease in carotid intima-media thickness after 1-year therapy with etidronate for osteopenia associated with type 2 diabetes. J Clin Endocrinol Metab. 2000;85(8):2793–6. doi: 10.1210/jcem.85.8.6748. [DOI] [PubMed] [Google Scholar]
- 32.Ylitalo R, Kalliovalkama J, Wu X, Kankaanranta H, Salenius JP, Sisto T, Lahteenmaki T, Ylitalo P, Porsti I. Accumulation of bisphosphonates in human artery and their effects on human and rat arterial function in vitro. Pharmacol Toxicol. 1998;83(3):125–31. doi: 10.1111/j.1600-0773.1998.tb01455.x. [DOI] [PubMed] [Google Scholar]
- 33.Wermers RA, Khosla S, Atkinson EJ, Grant CS, Hodgson SF, O'Fallon WM, Melton LJ., 3rd Survival after the diagnosis of hyperparathyroidism: a population-based study. Am J Med. 1998;104(2):115–22. doi: 10.1016/s0002-9343(97)00270-2. [DOI] [PubMed] [Google Scholar]
- 34.Steingrimsdottir L, Gunnarsson O, Indridason OS, Franzson L, Sigurdsson G. Relationship between serum parathyroid hormone levels, vitamin D sufficiency, and calcium intake. Jama. 2005;294(18):2336–41. doi: 10.1001/jama.294.18.2336. [DOI] [PubMed] [Google Scholar]