

Abstract
Although mice deficient in various genes are providing greater insight into the mechanisms of restenosis after angioplasty, there have been limitations with murine models not simulating human vascular disease. To develop a more clinically applicable model of primary atherosclerosis and restenosis following angioplasty of the primary lesion, we fed apolipoprotein E-deficient mice a Western diet and occluded the left common carotid artery for 2 days. Three weeks after flow was restored, the temporarily occluded carotids demonstrated atherosclerotic lesions containing foam cells, cholesterol clefts, necrotic cores, and fibrous capsules. The atherosclerotic carotids in other animals underwent angioplasty with a beaded probe, resulting in plaque and medial layer disruption. Three weeks after angioplasty, although there was significant neointimal lesion formation, the luminal narrowing did not change significantly secondary to overall vessel enlargement (positive remodeling). Neointimal lesions were composed of smooth-muscle cells and extracellular matrix observed adjacent to the original atherosclerotic plaques. Similarly, even at 3 months after the angioplasty the lumen was maintained despite greater neointimal lesion formation caused by progressive positive remodeling. This new murine model of primary atherosclerosis and postangioplasty intimal hyperplasia and remodeling mimics the human disease pattern of postangioplasty intimal hyperplasia. Used in transgenic animals, this model will likely facilitate understanding of the mechanisms of restenosis in humans.
Percutaneous transluminal coronary angioplasty and stenting have become the first-line treatment for symptomatic coronary artery disease. Despite recent advances in technology, however, up to 50% of patients have recurrence of symptoms because of intimal hyperplasia and arterial remodeling in the treated arteries. 1,2 To obtain insights into the structural and cellular mechanisms leading to restenosis, many animal models (ie, pig, rabbit, rat) have been developed using mechanical, electrical, and chemical injuries to arteries. In particular, the potential for genetic manipulations in mice has made these especially important to identify the key molecules involved in restenosis. 3
Nevertheless, current murine models are limited because they often do not reflect the pathophysiology of human restenosis. For instance, injury to normal, nonatherosclerotic arteries fails to consider the proper importance of the underlying atherosclerosis to pathways that contribute to restenosis in humans. 4-7 Furthermore, many models do not specifically address the adaptive remodeling after arterial injury, which has a significant role in the pathogenesis of human restenosis. 8 Therefore, a mouse model of restenosis should include arteries with atherosclerotic plaques that bear maximum similarity to the human disease and should mimic neointimal lesion formation and adaptive remodeling, the two paradigms of restenosis after angioplasty.
We have developed a model in mice that meets these conditions. By inducing primary and secondary injuries in mice deficient in apolipoprotein E (ApoE-KO), we have recapitulated the human conditions in which restenosis occurs in response to injury of arteries with pre-existing advanced atherosclerosis. Our approach involves induction of a primary atherosclerotic-like lesion in the carotid artery comprising the entire range of morphological features observed in mature human atheroma including foam cells, cholesterol clefts, necrotic cores, and fibrous capsules. Next, the carotid atherosclerotic lesion undergoes intraluminal dilatation (angioplasty) resulting in morphology typical of the neointimal lesion formation and remodeling observed after balloon angioplasty of human coronaries as documented by the Serial Ultrasound Restenosis (SURE) study. 9 The new murine model developed should facilitate understanding of the effects of specific proteins and pathways involved in the secondary intimal hyperplasia and vascular remodeling that results from intervention.
Materials and Methods
Experimental Design and Animals
The experimental design is summarized in Figure 1A ▶ . Animal procedures were approved by the Animal Studies Committee at Washington University. Forty-six, 10- to 12-week-old ApoE-KO mice (C57BL/6 background; Jackson Laboratories, Bar Harbor, ME) were bred in-house. The animals were weaned at 4 weeks and fed normal chow. One week before the first surgery (temporary ligation), the animals were started on Western-type diet (42% of total calories from fat, 0.15% cholesterol; Harlan-Teklad, Madison, WI). The animals were returned to normal chow on the day of the second surgery (probe angioplasty). Anesthesia for all surgeries was induced by intraperitoneal injection of Ketamine (80 mg/kg) and Xylazine (5 mg/kg).
Figure 1.

Schematic of the experimental protocol and representative cross-sections of vessels collected at the four major intervals in the study. A: Timeline of diets and procedures on vessels. Animals were fed a western diet for 1 week and then underwent carotid ligation. Two days later, the ligature was removed, restoring blood flow in the carotid artery. B: Atherosclerotic lesion in the narrowest lumen 3 weeks after removal of the carotid ligature (magnification, ×200). C: Atherosclerotic lesion in the narrowest lumen immediately after angioplasty (×200). D: Neointimal lesion in the narrowest lumen 3 weeks after probe angioplasty (×200). E: Lesions 3 months after probe angioplasty (×200).
The animals were divided into four groups to demonstrate the different stages of the vascular response: 1) primary atherosclerotic lesion, 2) primary lesion immediately after probe angioplasty, 3) neointimal lesion 3 weeks after probe angioplasty, and 4) neointimal lesion 3 months after angioplasty. In detail, all animals underwent left carotid artery exposure and placement of a 6−0 silk suture around the mid-common carotid artery, which was cinched tight with a small titanium clip (catalog number 523835; Edward Weck and Co., Research Triangle Park, NC) to stop blood flow. An additional 9 animals underwent a sham operation, but the artery was not ligated. The skin was closed with a 4−0 silk suture. Forty-eight hours later, the ligature was removed to restore blood flow. After 3 weeks, 11 animals were selected randomly for sacrifice and vessels were perfusion-fixed for analysis of the primary atherosclerotic lesions (Figure 1B) ▶ .
The remaining animals with atherosclerotic lesions underwent intraluminal dilatation with a wire probe (probe angioplasty). We made the probe by attaching an epoxy bead (0.57 mm in diameter) to a 0.014-inch-diameter wire using an aluminum mold. The mold was created using two halves of an aluminum block (2 cm3) and a Dremel tool with a tungsten carbide cutter (catalog number 9909; Dremel Inc., Racine, WI). The egg-shaped mold was cut to a maximum diameter of 0.57 mm (approx. 150% of the diameter of the mouse common carotid artery). The aluminum blocks were then sprayed with mold release 3M silicone lubricant (3M Electrical Product, Austin, TX). One drop of Scotchcast 9 electrical epoxy resin (3M Electric Product) was placed in each half of the mold, and a stainless steel music wire (0.014-inch diameter; McMaster-Carr, Chicago, IL) was then placed in the middle of the mold. The blocks were pressed together with a C-clamp for 24 hours. The probe was removed and polished with a Dremel polishing wheel (number 520; Dremel Inc.).
The probe was inserted into the external carotid artery and passed retrograde three times into the common carotid artery proximal to the primary atherosclerotic lesion. The probe increased the lumen size of the narrowed artery by overstretching and denuding the endothelium from the vessel mimicking the mechanisms of balloon angioplasty. Immediately after angioplasty, the vessels from 11 animals were perfusion-fixed and analyzed for the effectiveness of the angioplasty (Figure 1C) ▶ . At 3 weeks and at 3 months, the carotids vessels of 10 and 9 animals, respectively, were perfusion-fixed and analyzed for the development of maximum narrowing secondary to intimal hyperplasia and remodeling (Figure 1D) ▶ .
Measurement of Serum Cholesterol Levels
Before perfusion-fixation, blood was drawn from the right ventricle for analysis of cholesterol levels with use of an Affinity Cholesterol Reagent Procedure (number 402; ς-Aldrich, St. Louis, MO). Standards were prepared from a Cholesterol Standard Solution, 200 mg/dL (Wako Chemicals, Neuss, Germany).
Histology, Immunohistochemistry, and Morphometry
The carotid arteries were perfusion-fixed in situ at 100 mm Hg with 10% formalin in PBS delivered for 4 minutes through a catheter in the left ventricle. The entire left common carotid artery was paraffin-embedded, and cross-sections (5 μm) were taken every 100 μm from the aortic arch to the carotid bifurcation (approximately 20 to 25 sections). All 20 to 25 sections were stained with Verhoeff’s van Gieson elastin stain and analyzed to determine the minimum lumen area (narrowest segment) for each carotid artery. This narrowest lumen area was always at the mid-carotid artery level where the ligature had been placed temporarily. We wanted to mimic the characterization of diseased arteries in humans, where the entire artery is often defined by its maximum narrowing. Therefore, we also analyzed the mouse carotid arteries by their maximum narrowing. Once the section with the smallest lumen from each vessel was determined, these sections were compared among the stages of lesion development. 10 For immunohistochemistry, selected sections were stained for smooth-muscle cells (SM-specific α-actin, 1:500 dilution; ς-Aldrich) and for macrophages (Mac-3, 1:1000 dilution; PharMingen, San Diego, CA).
The immunohistochemical protocol, including negative controls, is described elsewhere. 11 Briefly, slides were rinsed in PBS for 30 minutes and 1% hydrogen peroxide/PBS for 30 minutes and were then treated with citrate buffer solution (pH 6) in a pressure cooker at 15 psi for 3 minutes followed by a fresh solution for 3 minutes. Slides were treated with avidin/biotin blocking (SP-2001; Vector Laboratories) for 20 minutes and with protein block (X0909; Dako, Carpenteria, CA) for 10 minutes. Primary antibody was incubated for 1 hour at 30°C. After a 10-minute PBS rinse, secondary antibody was applied (biotinylated goat anti-rat IgG, 1:1000 dilution; Accurate Chemical & Scientific Corp., Westbury, CA; or biotinylated goat anti-mouse IgG, 1:800 dilution; Vector Laboratories) for 30 minutes at 30°C. Slides were then incubated with SA-HRP (P0307, 1: 1000; Dako) for 30 minutes and with DAB (D-9015; ς-Aldrich) until staining was evident microscopically. Sections were counterstained with hematoxylin.
Morphometric measurements for luminal, intimal, medial, and total vascular areas of the section with the smallest lumen were performed on digitized images of the Verhoeff’s van Gieson-stained sections with use of Olympus Microsuite software (Soft Imaging Systems, Munster, Germany). Measured total vascular area was determined as the area inside the external elastic lamina (EEL), while calculated total vascular area was calculated from the EEL circumference.
Statistical Analysis
Lesion characteristics were compared by analysis of variance and Student’s t-test (Microsoft Office Excel 2000). Data are presented as mean ± SEM unless otherwise noted. Probability values of P < 0.05 were considered significant.
Results
Primary Atherosclerosis
Forty-one of 46 animals completed the protocol and were analyzed. All animals subjected to temporary carotid ligation and reflow had atherosclerotic lesions after 3 weeks. Morphometric analysis demonstrated a narrowest luminal area of 0.042 ± 0.014 mm2 and corresponding intimal plaque area of 0.047 ± 0.018 mm2 at 3 weeks (Table 1) ▶ . In comparison, the sham-operated Apo E-KO mice (n = 9) had a luminal area of 0.043 ± 0.015 mm2 (no significant difference) and no intimal plaque. The luminal area was maintained in the temporary ligation group despite the development of atherosclerotic plaque secondary to its total vessel enlargement (0.136 ± 0.016 mm2) compared to the sham group (0.082 ± 0.010 mm2; P < 0.01). Equal numbers of male and female ApoE-KO mice were used for all groups, and there were no significant gender differences in any of the analyses (data not shown). Atherosclerotic lesions displayed the typical complex morphological features and heterogeneous cellular composition of atherosclerosis consisting of a fibrous cap, foam cells, cholesterol crystal clefts, and a necrotic core (Figure 1B ▶ ; Figure 2 ▶ ).
Table 1.
Cross-Sectional Area Measurements of ApoE-KO Mouse Carotid Arteries at the Narrowest Segment Before and After Angioplasty
| Primary athero (n = 11) | Immed. PA (n = 11) | 3 weeks PA (n = 10) | 3 months PA (n = 9) | |
|---|---|---|---|---|
| Lumen | 0.042 ± 0.014 | 0.050 ± 0.008 | 0.045 ± 0.019 | 0.053 ± 0.010 |
| Intima | 0.047 ± 0.018 | 0.015 ± 0.007* | 0.066 ± 0.027† | 0.110 ± 0.019‡ |
| Media | 0.046 ± 0.007 | 0.043 ± 0.007 | 0.063 ± 0.011† | 0.050 ± 0.011 |
| Intima + media | 0.094 ± 0.019 | 0.058 ± 0.012* | 0.129 ± 0.029† | 0.160 ± 0.023 |
| Total vessel (measured) | 0.136 ± 0.016 | 0.108 ± 0.010* | 0.174 ± 0.031† | 0.213 ± 0.024‡ |
| Total vessel (calculated)§ | 0.197 ± 0.019 | 0.154 ± 0.021* | 0.219 ± 0.025† | 0.285 ± 0.037‡ |
*P <0.05 versus primary athero.
†P <0.05 versus immed. PA.
‡P <0.05 versus 3 weeks PA.
§Calculated area using EEL circumference.
PA, post-angioplasty.
All measurements are mm2.
Figure 2.
Morphological features of the primary atherosclerotic lesions in mouse carotid arteries. A: Foam cells. B: Necrotic core. C: Cholesterol crystal clefts. D: Fibrous cap. Bar, 40 μm.
Probe Angioplasty
Probe angioplasty resulted consistently in intimal plaque and medial layer disruption (Figure 1D) ▶ . Immediately after angioplasty, the intimal plaque area decreased (0.015 ± 0.007 mm2; P < 0.05), but luminal area remained unchanged (0.050 ± 0.008 mm2; no significant difference) (Table 1) ▶ . Total vessel area was smaller immediately after angioplasty demonstrating that the reason the luminal area remained unchanged was due to a reduction in intimal plaque from the angioplasty.
Three weeks after angioplasty, there was significant neointimal lesion formation (0.066 ± 0.027 mm2, P < 0.05) with unchanged luminal area of 0.045 ± 0.019 mm2 (no significant difference). Despite an immediate reduction of the total vessel area after angioplasty, there was significant vessel enlargement at 3 weeks (0.174 ± 0.031 mm2; P < 0.05). The thickened neointima 3 weeks after angioplasty was characterized by accumulation of smooth muscle cells and matrix proteins (Figure 3A) ▶ . Mac-3 stained mononuclear cells were present preferentially in the media and in the old intimal plaque but not in the neointimal lesion (Figure 3) ▶ . Even at 3 months after angioplasty, the luminal area was maintained at 0.053 ± 0.010 mm2 despite a further significant increase in neointima (0.110 ± 0.019 mm2; P < 0.05) due to progressive enlargement of the total vessel area (Table 1) ▶ .
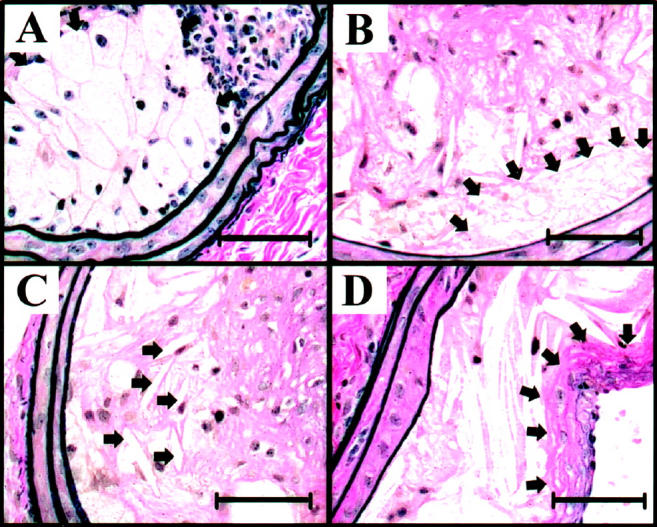
Figure 3.

Representative immunohistochemical staining for smooth-muscle cells (SMC) and macrophages of postangioplasty intimal lesions. A and C: Low- and high-power (inset) staining for SMC-specific α-actin demonstrating densely populated SMCs (brown) in the neointimal lesion and in the media (magnifications, ×200 and ×400, respectively). B and D: Low- and high-power (inset) staining for Mac-3 demonstrating macrophages (black) localized to the atherosclerotic intima (*, cholesterol clefts) sparing the neointimal lesion (×200 and ×400).
Serum Cholesterol Level
The baseline cholesterol level of ApoE-KO mice on regular chow diet was 496 ± 93 mg/dl. At the time of angioplasty, 4 weeks after starting Western-type diet, the serum cholesterol level had increased to 972 ± 176 mg/dl. Three months after resuming regular chow diet at the time of angioplasty, serum cholesterol levels had decreased to 496 ± 186 mg/dl.
Discussion
Despite availability of numerous animal models of atherosclerosis and angioplasty, none have thus far yielded data predictive of the outcome in clinical trials. 12,13 Drugs found effective for attenuating neointimal thickening after arterial injury in rodents have not been reproduced in humans, leading to the presumption that larger animal models (eg, pigs and nonhuman primates) were required to simulate conditions of human disease. The results of the present study show that the complex nature of restenosis after angioplasty is reasonably simulated with a double injury preparation in ApoE-KO mice. Probe angioplasty of an ApoE-KO mouse carotid artery with induced atherosclerotic-like lesions resulted in a response that shares many morphological characteristics with the response observed in patients undergoing coronary angioplasty.
The first step to mimic the responses to clinical angioplasty was to induce atherosclerotic-like lesions in an accessible vessel. Primary atherosclerotic lesions generated 3 weeks after temporary carotid artery ligation resembled the advanced, complex atherosclerotic plaques that are treated with angioplasty (Figure 1B ▶ ; Figure 2 ▶ ). Our approach has several advantages over the de novo generation of atherosclerotic plaques in ApoE-KO mice fed Western diet alone. 13 Temporary ligation yielded a significant luminal narrowing, and the lesion was more advanced with inclusion of foam cells, cholesterol clefts, necrotic cores, and fibrous caps than the de novo plaques produced by diet alone (Figure 2) ▶ . 14,15 In addition, our approach generated a significant atherosclerotic plaque in 3 weeks compared to 6 to 12 months needed for plaque development on high-fat diet alone. Moreover, diet-induced plaques are not always amenable to angioplasty due to the remote locations (eg, aortic sinus, coronary arteries) of lesions. 16 With the exception of the 2 days of the ligation, flow through the carotid artery was maintained throughout the experiment. Consistent with the observations of Kawasaki et al, 17 2 days of temporary ligation was not enough time to induce chronic occlusion of the carotid artery.
Once the primary atherosclerotic plaque was generated, probe angioplasty was performed, resulting in acute dilatation of the arterial wall, plaque fracture, dissection, and occasionally medial fracture or delamination (Figure 1C) ▶ , thereby reproducing the results of balloon angioplasty in human atherosclerotic vessels. 18 In fact, the noncompressible probe used here may more closely resemble the rigid Gruentzig-type angioplasty balloon used in humans compared to the compressible Fogarty balloon used almost universally in experimental animals. More importantly, the probe angioplasty resulted in reduction of intimal plaque and medial area by 38% in the narrowest luminal segment (Table 1) ▶ . As demonstrated in the SURE study, 9 the total plaque and medial area decreased by 15% immediately after balloon angioplasty. However, the human total vessel area increased immediately after balloon angioplasty while the mouse carotid total vessel area decreased immediately after angioplasty. Indeed, the human study revealed that the immediate effect of the balloon angioplasty was luminal enlargement due to both a reduction in plaque and medial area and total vessel enlargement. In the mouse, the lumen size did not change after angioplasty due to a reduction in plaque and medial area but also a reduction in total vessel area.
From the time of probe angioplasty, the animals were removed from the Western diet to reduce further deposition of cholesterol at the plaque site and to generate a densely cellular intimal hyperplastic lesion analogous to the neointimal thickening seen in human restenosis. We have observed that continued high-fat diet after the second injury induces intimal lesions that resemble fatty streaks and not the typical hypercellular, fibrotic intimal lesions seen with restenosis in humans (not shown). Only when we stopped the high-fat diet did the neointimal lesion resemble the human intimal hyperplastic lesion. Indeed, 3 weeks after probe angioplasty, neointimal lesion development was quite significant (Table 1) ▶ . Figure 3A ▶ shows smooth-muscle cells were the predominant cell type in the neointima. Neointimal Mac-3 staining macrophages were minimal (Figure 3) ▶ similar to the description of human intimal hyperplasia by Dr. Bruce Waller 18,19 : “smooth muscle cells and intimal fibrous proliferation coating the surrounding portions of atherosclerotic plaque in addition to the area of previous plaque fracture, producing a severely narrowed coronary artery.” Thus, the restenotic intima is distinctly different from the primary atherosclerotic intima, which has less smooth-muscle cells and more macrophage-derived foam cells. 20
In addition to the neointimal growth following probe angioplasty, there was total vessel enlargement after 3 weeks (Table 1) ▶ . We compared the vascular remodeling response of the present mouse model to the results of the SURE study (balloon angioplasty of human coronary). 9 At 1 month after balloon angioplasty, the SURE study showed that total vessel area was 128% of the pre-angioplasty area as estimated by intravascular ultrasound resulting in a 28% expansive remodeling. Similarly, in the present mouse model there was a 28% expansive remodeling at 3 weeks postangioplasty (Figure 4) ▶ . However, at 3 months postangioplasty, the mouse carotid had progressive total vessel enlargement by 56%. In contrast, at 6 months postangioplasty, the human total vessel area diminished to 108% of the pre-angioplasty area. The mouse data at 6 months postangioplasty are not yet available. Figure 4 ▶ also shows the preservation of the lumen in both mice and humans. Unexpectedly, there does not appear to be any neointimal lesion formation postangioplasty in the human coronary. In the mouse, however, we saw progressive neointimal lesion formation even at 3 months postangioplasty. It is unclear why in the SURE study there was minimal neointimal hyperplasia seen postangioplasty.
Figure 4.
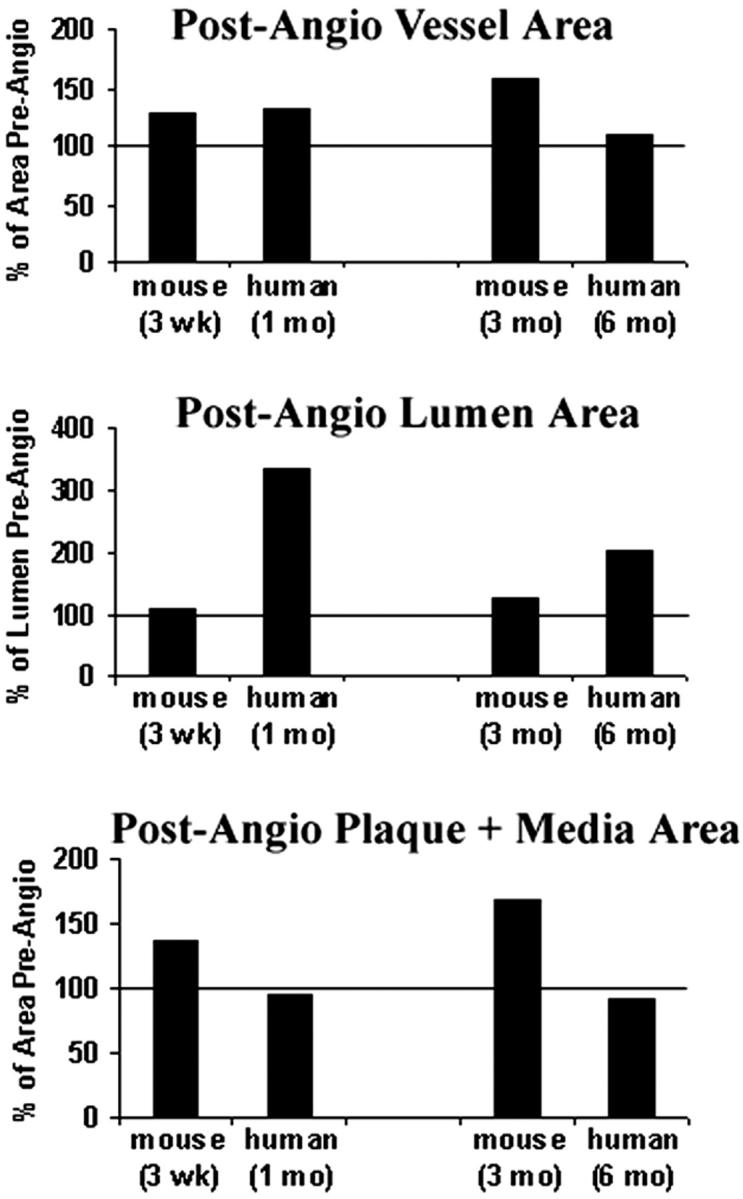
Comparison of total vessel area (measured), luminal area and plaque + media area after angioplasty in mice and humans. 9 The postangioplasty areas presented in percentages are compared to the corresponding areas before angioplasty.
Overall, the double injury preparation in Apo E-KO mouse appears to mimic human disease quite closely while keeping experiments within a short timeframe. Nevertheless, there are some limitations. Induction of double injuries is more time-consuming than single injuries producing intimal thickening in otherwise normal arteries. In addition, the mortality of mice undergoing three procedures under general anesthesia is higher at 10% to 15% in our series. However, the mortality rate is likely to decrease with experience. As coronary stenting surpasses balloon angioplasty alone as the preferred mode of therapy, this model must be modified to be a useful animal model of carotid stenting. There is also a significant variability in lesion formation and remodeling in all animal models, including this one. By determining the maximum narrowing in mouse carotids, as we do with human coronary lesions, we were able to find significant differences from time point to time point after angioplasty with 9 to 11 animals per group. However, to find more subtle differences between transgenic and wild-type animals, we may need to increase the size of groups.
A large number of double-knockout or transgenic mice involving the ApoE gene are already available and will be ideal to study the complex nature of restenosis following angioplasty. Moreover, the model will permit comparisons of the findings in genetically altered animals with those obtained using blocking antibodies or other antagonists, which may be difficult to accomplish in larger animals.
Acknowledgments
We thank the Washington University Digestive Disease Research Cores Center Morphology Core for assistance with preparation of histological sections.
Footnotes
Address reprint requests to Eric T. Choi, M.D., Section of Vascular Surgery, 660 S. Euclid Ave., Campus Box 8109, St. Louis, MO 63110. E-mail: [email protected].
Supported in part by the American Heart Association (Beginning Grant-in-Aid from AHA Heartland Affiliate, Inc. to E.T.C.) and the National Institutes of Health (grant P30 DK52514; grant K08 HL-68119 to E.T.C., and R01 HL-48762 to W.C.P.).
References
- 1.Teirstein PS: Living the dream of no restenosis. Circulation 2001, 104:1996-1998 [PubMed] [Google Scholar]
- 2.Smith SC, Jr., Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, Kuntz RE, Popma JJ, Schaff HV, Williams DO, Gibbons RJ, Alpert JP, Eagle KA, Faxon DP, Fuster V, Gardner TJ, Gregoratos G, Russell RO: ACC/AHA guidelines for percutaneous coronary intervention (revision of the 1993 PTCA guidelines): executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty) endorsed by the Society for Cardiac Angiography and Interventions. Circulation 2001, 103:3019-3041 [DOI] [PubMed] [Google Scholar]
- 3.Smith JD, Breslow JL: The emergence of mouse models of atherosclerosis and their relevance to clinical research. J Intern Med 1997, 242:99-109 [DOI] [PubMed] [Google Scholar]
- 4.Ross R: Atherosclerosis: an inflammatory disease. N Engl J Med 1999, 340:115-126 [DOI] [PubMed] [Google Scholar]
- 5.Kumar A, Lindner V: Remodeling with neointima formation in the mouse carotid artery after cessation of blood flow. Arterioscler Thromb Vasc Biol 1997, 17:2238-2244 [DOI] [PubMed] [Google Scholar]
- 6.Carmeliet P, Moons L, Stassen JM, De Mol M, Bouche A, van den Oord JJ, Kockx M, Collen D: Vascular wound healing and neointima formation induced by perivascular electric injury in mice. Am J Pathol 1997, 150:761-776 [PMC free article] [PubMed] [Google Scholar]
- 7.Roque M, Fallon JT, Badimon JJ, Zhang WX, Taubman MB, Reis ED: Mouse model of femoral artery denudation injury associated with the rapid accumulation of adhesion molecules on the luminal surface and recruitment of neutrophils. Arterioscler Thromb Vasc Biol 2000, 20:335-342 [DOI] [PubMed] [Google Scholar]
- 8.Glagov S: Intimal hyperplasia, vascular modeling, and the restenosis problem. Circulation 1994, 89:2888-2891 [DOI] [PubMed] [Google Scholar]
- 9.Kimura T, Kaburagi S, Tamura T, Yokoi H, Nakagawa Y, Hamasaki N, Nosaka H, Nobuyoshi M, Mintz GS, Popma JJ, Leon MB: Remodeling of human coronary arteries undergoing coronary angioplasty or atherectomy. Circulation 1997, 96:475-483 [DOI] [PubMed] [Google Scholar]
- 10.Choi ET, Callow AD, Sehgal NL, Brown DM, Ryan US: Halofuginone, a specific collagen type I inhibitor, reduces anastomotic intimal hyperplasia. Arch Surg 1995, 130:257-261 [DOI] [PubMed] [Google Scholar]
- 11.Choi ET, Engel L, Callow AD, Sun S, Trachtenberg J, Santoro S, Ryan US: Inhibition of neointimal hyperplasia by blocking αVβ3 integrin with a small peptide antagonist GpenGRGDSPCA. J Vasc Surg 1994, 19:125-134 [DOI] [PubMed] [Google Scholar]
- 12.Casterella PJ, Teirstein PS: Prevention of coronary restenosis. Cardiol Rev 1999, 7:219-231 [DOI] [PubMed] [Google Scholar]
- 13.Wang X, Paigen B: Comparative genetics of atherosclerosis and restenosis: exploration with mouse models. Arterioscler Thromb Vasc Biol 2002, 22:884-886 [DOI] [PubMed] [Google Scholar]
- 14.Jonasson L, Holm J, Skalli O, Bondjers G, Hansson GK: Regional accumulations of T cells, macrophages, and smooth-muscle cells in the human atherosclerotic plaque. Arteriosclerosis 1986, 6:131-138 [DOI] [PubMed] [Google Scholar]
- 15.Xu QB, Oberhuber G, Gruschwitz M, Wick G: Immunology of atherosclerosis: cellular composition and major histocompatibility complex class II antigen expression in aortic intima, fatty streaks, and atherosclerotic plaques in young and aged human specimens. Clin Immunol Immunopathol 1990, 56:344-359 [DOI] [PubMed] [Google Scholar]
- 16.Zhang SH, Reddick RL, Piedrahita JA, Maeda N: Spontaneous hypercholesterolemia and arterial lesions in mice lacking apolipoprotein E. Science 1992, 258:468-471 [DOI] [PubMed] [Google Scholar]
- 17.Kawasaki T, Dewerchin M, Lijnen HR, Vreys I, Vermylen J, Hoylaerts MF: Mouse carotid artery ligation induces platelet-leukocyte-dependent luminal fibrin, required for neointima development. Circ Res 2001, 88:159-166 [DOI] [PubMed] [Google Scholar]
- 18.Waller BF, Orr CM, Slack JD, Pinkerton CA, Van Tassel J, Peters T: Anatomy, histology, and pathology of coronary arteries: a review relevant to new interventional and imaging techniques: part II. Clin Cardiol 1992, 15:535-540 [DOI] [PubMed] [Google Scholar]
- 19.Waller BF: Pathology of transluminal balloon angioplasty used in the treatment of coronary heart disease. Cardiol Clin 1989, 7:749-770 [PubMed] [Google Scholar]
- 20.Schwartz SM, de Blois D, O’Brien ER: The intima: soil for atherosclerosis and restenosis. Circ Res 1995, 77:445-465 [DOI] [PubMed] [Google Scholar]